Liabeuf Sophie, Desjardins Lucie, Diouf Momar, Temmar Mohamed, Renard Cédric, Choukroun Gabriel, Massy Ziad A
INSERM U1088, Jules Verne University of Picardy Amiens, France; Clinical Research Centre and Division of Clinical Pharmacology, Amiens University Hospital and the Jules Verne University of Picardy, Amiens, France.
Department of Biostatistics, Amiens University Hospital, Amiens, France.
PLoS One. 2015 Jul 16;10(7):e0131707. doi: 10.1371/journal.pone.0131707. eCollection 2015.
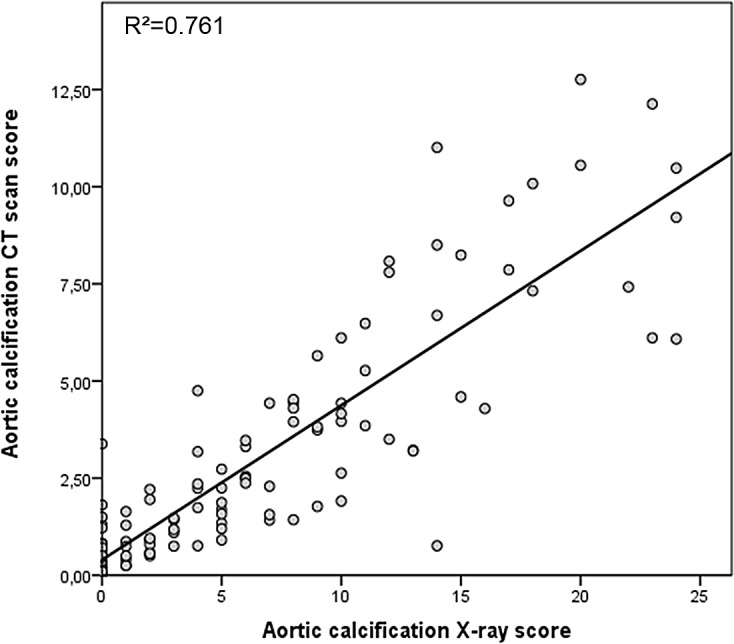
Although a variety of non-invasive methods for measuring cardiovascular (CV) risk (such as carotid intima media thickness, pulse wave velocity (PWV), coronary artery and aortic calcification scores (measured either by CT scan or X-ray) and the ankle brachial index (ABI)) have been evaluated separately in chronic kidney disease (CKD) cohorts, few studies have evaluated these methods simultaneously. Here, we looked at whether the addition of non-invasive methods to traditional risk factors (TRFs) improves prediction of the CV risk in patients at different CKD stages.
We performed a prospective, observational study of the relationship between the outputs of non-invasive measurement methods on one hand and mortality and CV outcomes in 143 patients at different CKD stages on the other. During the follow-up period, 44 patients died and 30 CV events were recorded. We used Cox models to calculate the relative risk for outcomes. To assess the putative clinical value of each method, we also determined the categorical net reclassification improvement (NRI) and the integrated discrimination improvement.
Vascular calcification, PWV and ABI predicted all-cause mortality and CV events in univariate analyses. However, after adjustment for TRFs, only aortic and coronary artery calcification scores were found to be significant, independent variables. Moreover, the addition of coronary artery calcification scores to TRFs improved the specificity of prediction by 20%.
The addition of vascular calcification scores (especially the coronary artery calcification score) to TRFs appears to improve CV risk assessment in a CKD population.
尽管多种用于测量心血管(CV)风险的非侵入性方法(如颈动脉内膜中层厚度、脉搏波速度(PWV)、冠状动脉和主动脉钙化评分(通过CT扫描或X射线测量)以及踝臂指数(ABI))已在慢性肾脏病(CKD)队列中分别进行了评估,但很少有研究同时评估这些方法。在此,我们研究了在传统风险因素(TRF)基础上增加非侵入性方法是否能改善不同CKD阶段患者CV风险的预测。
我们对143例不同CKD阶段患者进行了一项前瞻性观察研究,一方面观察非侵入性测量方法的结果,另一方面观察死亡率和CV结局之间的关系。在随访期间,44例患者死亡,记录到30例CV事件。我们使用Cox模型计算结局的相对风险。为评估每种方法的假定临床价值,我们还确定了分类净重新分类改善(NRI)和综合鉴别改善。
在单变量分析中,血管钙化、PWV和ABI可预测全因死亡率和CV事件。然而,在对TRF进行调整后,仅发现主动脉和冠状动脉钙化评分是显著的独立变量。此外,在TRF基础上增加冠状动脉钙化评分可使预测特异性提高20%。
在TRF基础上增加血管钙化评分(尤其是冠状动脉钙化评分)似乎可改善CKD人群的CV风险评估。