Toleva Olga, Ibrahim Quazi, Brass Neil, Sookram Sunil, Welsh Robert
University of Alberta , Edmonton, Alberta , Canada.
Royal Alexandra Hospital and CK Hui Heart Centre , Edmonton, Alberta , Canada.
Open Heart. 2015 Jun 24;2(1):e000235. doi: 10.1136/openhrt-2014-000235. eCollection 2015.
Management of elderly patients with ST elevation myocardial infarction (STEMI) is challenging and they are under-represented in trials. Accordingly, we analysed reperfusion strategies and their effectiveness in patients with STEMI ≥75 years compared to <75 years within a comprehensive inclusive registry.
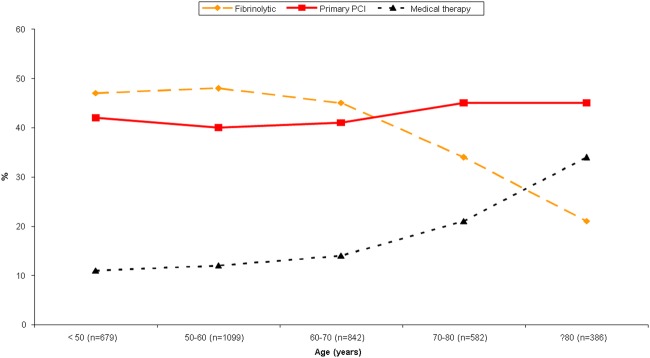
Consecutive patients with STEMI admitted to hospital and tracked within a regional registry (2006-2011) were analysed comparing reperfusion strategy (primary percutaneous coronary intervention (PPCI), fibrinolysis and no reperfusion) between patients ≥75 vs <75 years old as well as across the reperfusion strategies in those ≥75 years.
There were 3588 patients with STEMI with 646 (18%) ≥75 years old. Elderly patients were more likely female (46.9% vs 18.4%) and had more prior: angina (28.2% vs 17.2%), myocardial infarction (MI; 22.8% vs 13.9%), hypertension (67.6% vs 44.2%), heart failure (2.3% vs 0.3%) and atrial fibrillation (2.2% vs 0.5%) (all p<0.001). The reperfusion strategy for patients ≥75 vs <75: PPCI 45.3% vs 41.2%, fibrinolysis 24.8% vs 45.7%, and no reperfusion 29.9% vs 13.1% (p<0.001). Time from symptoms to first medical contact (median, 93 vs 78 min p=0.008) and PPCI (median, 166 vs 136 min (p<0.001) were longer for ≥75 years. In those ≥75 years outcomes by reperfusion (PPCI, fibrinolysis and none) were: in-hospital death 13.3%, 9.4% and 19.7% (p=0.018), and composite of death, recurrent-MI, cardiogenic shock and congestive heart failure 28%, 20% and 33.2% (p=0.022).
Elderly patients have more comorbidities, worst in-hospital clinical outcomes and are less likely to receive reperfusion. Acknowledging physician selection of the reperfusion strategy; outcomes appear favourable in the elderly receiving fibrinolysis.
老年ST段抬高型心肌梗死(STEMI)患者的管理具有挑战性,且他们在试验中的代表性不足。因此,我们在一个全面的包容性登记系统中,分析了年龄≥75岁与<75岁的STEMI患者的再灌注策略及其有效性。
分析2006 - 2011年期间在区域登记系统中连续入院并被追踪的STEMI患者,比较年龄≥75岁与<75岁患者的再灌注策略(直接经皮冠状动脉介入治疗(PPCI)、溶栓治疗和未进行再灌注治疗),以及年龄≥75岁患者不同再灌注策略的情况。
共有3588例STEMI患者,其中646例(18%)年龄≥75岁。老年患者女性比例更高(46.9%对18.4%),既往有更多的心绞痛(28.2%对17.2%)、心肌梗死(MI;22.8%对13.9%)、高血压(67.6%对44.2%)、心力衰竭(2.3%对0.3%)和心房颤动(2.2%对0.5%)(所有p<0.001)。年龄≥75岁与<75岁患者的再灌注策略:PPCI分别为45.3%对41.2%,溶栓治疗分别为24.8%对45.7%,未进行再灌注治疗分别为29.9%对13.1%(p<0.001)。年龄≥75岁患者从症状出现到首次医疗接触的时间(中位数,93分钟对78分钟,p = 0.008)和PPCI时间(中位数,166分钟对136分钟,p<0.001)更长。在年龄≥75岁的患者中,不同再灌注治疗(PPCI、溶栓治疗和未治疗)的结果如下:住院死亡率分别为13.3%、9.4%和19.7%(p = 0.018),死亡、再发心肌梗死、心源性休克和充血性心力衰竭的复合发生率分别为28%、20%和33.2%(p = 0.022)。
老年患者合并症更多,住院临床结局更差,接受再灌注治疗的可能性更小。考虑到医生对再灌注策略的选择;老年患者接受溶栓治疗的结局似乎较好。