Leeper Heather E, Caron Alissa A, Decker Paul A, Jenkins Robert B, Lachance Daniel H, Giannini Caterina
Neuro-Oncology, Advocate Medical Group, Park Ridge, IL 60068, USA.
Experimental Pathology, Mayo Clinic SW, Rochester, MN 55905, USA.
Oncotarget. 2015 Oct 6;6(30):30295-305. doi: 10.18632/oncotarget.4497.
Epigenetic, genetic, and molecular studies have identified several diagnostic and prognostic markers in diffuse gliomas. Their importance for evaluating WHO grade II gliomas has yet to be specifically delineated.
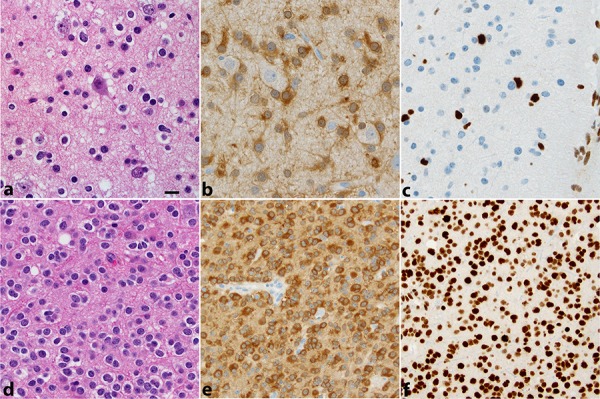
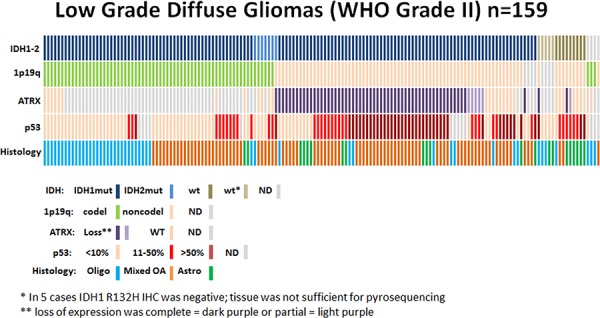
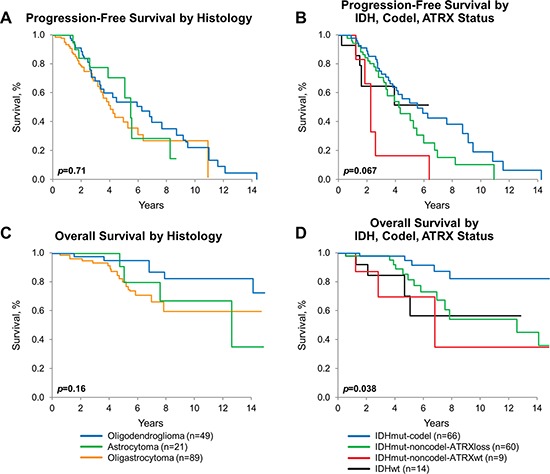
We analyzed markers, including IDH mutation(IDHmut), 1p19q codeletion(1p19qcodel), ATRX expression loss(ATRX loss) and p53 overexpression, and outcomes in 159 patients with WHO grade II oligodendroglioma, oligoastrocytoma, and astrocytoma (2003-2012).
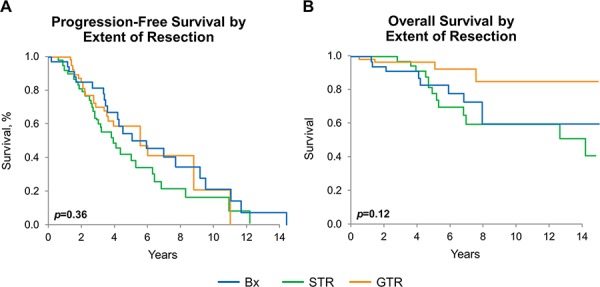
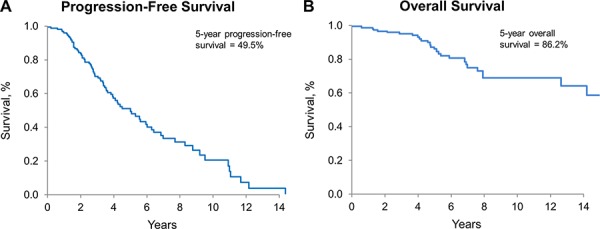
IDHmut was found in 141(91%) and ATRX loss in 64(87%) of IDHmut-noncodel tumors (p = 0.003). All codeleted tumors (n = 66) were IDHmut. Four subgroups were identified: IDHmut-codel, 66(43%); IDHmut-noncodel-ATRX loss, 60(39%); IDHmut-noncodel-ATRXwt, 9(6%); IDHwt, 14(9%). Median survival among 4 groups was significantly different (p = 0.038), particularly in IDHmut-codel (median survival 15.6 years) compared to the remaining 3 groups (p = 0.025). Survival by histology was not significant. Overall (OS), but not progression-free (PFS), survival was significantly longer with gross total resection vs. biopsy only (p = 0.042). Outcomes for patients with subtotal resection were not significantly different from those with biopsy only. Among these uniformly treated patients, OS far exceeds PFS, particularly in those with 1p/19q codeletion.
For WHO grade II diffuse glioma, molecular classification using 1p/19qcodel, IDHmut, and ATRX loss more accurately predicts outcome and should be incorporated in the neuropathologic evaluation.
表观遗传学、遗传学和分子学研究已在弥漫性胶质瘤中鉴定出多种诊断和预后标志物。它们对评估世界卫生组织(WHO)二级胶质瘤的重要性尚未明确界定。
我们分析了159例WHO二级少突胶质细胞瘤、少突星形细胞瘤和星形细胞瘤患者(2003 - 2012年)的标志物,包括异柠檬酸脱氢酶(IDH)突变(IDHmut)、1p19q共缺失(1p19qcodel)、α地中海贫血/智力低下综合征X连锁基因(ATRX)表达缺失(ATRX缺失)和p53过表达,以及预后情况。
在IDHmut非共缺失肿瘤中,141例(91%)发现IDHmut,64例(87%)发现ATRX缺失(p = 0.003)。所有共缺失肿瘤(n = 66)均为IDHmut。确定了四个亚组:IDHmut - 共缺失,66例(43%);IDHmut - 非共缺失 - ATRX缺失,60例(39%);IDHmut - 非共缺失 - ATRX野生型,9例(6%);IDH野生型,14例(9%)。四组患者的中位生存期有显著差异(p = 0.038),特别是IDHmut - 共缺失组(中位生存期15.6年)与其余三组相比(p = 0.025)。组织学类型的生存期无显著差异。总体生存期(OS),而非无进展生存期(PFS),与仅行活检相比,大体全切除患者显著更长(p = 0.042)。次全切除患者的预后与仅行活检患者无显著差异。在这些接受统一治疗的患者中,OS远超过PFS,尤其是在1p/19q共缺失患者中。
对于WHO二级弥漫性胶质瘤,使用1p/19qcodel、IDHmut和ATRX缺失进行分子分类能更准确地预测预后,应纳入神经病理学评估。