Kovari Helen, Russmann Stefan, Ledergerber Bruno, Müller Daniel, Rotger Margalida, Velli Pablo, Cavassini Matthias, Ambrosioni Juan, Bregenzer Andrea, Stöckle Marcel, Bernasconi Enos, Rauch Andri, Speck Roberto F
Division of Infectious Diseases and Hospital Epidemiology, University Hospital, University of Zurich, Zurich, Switzerland.
Department of Clinical Pharmacology and Toxicology, University Hospital Zurich, Zurich, Switzerland.
PLoS One. 2015 Jul 28;10(7):e0133879. doi: 10.1371/journal.pone.0133879. eCollection 2015.
Ribavirin (RBV) is an essential component of most current hepatitis C (HCV) treatment regimens and still standard of care in the combination with pegylated interferon (pegIFN) to treat chronic HCV in resource limited settings. Study results in HIV/HCV-coinfected patients are contradicting as to whether RBV concentration correlates with sustained virological response (SVR).
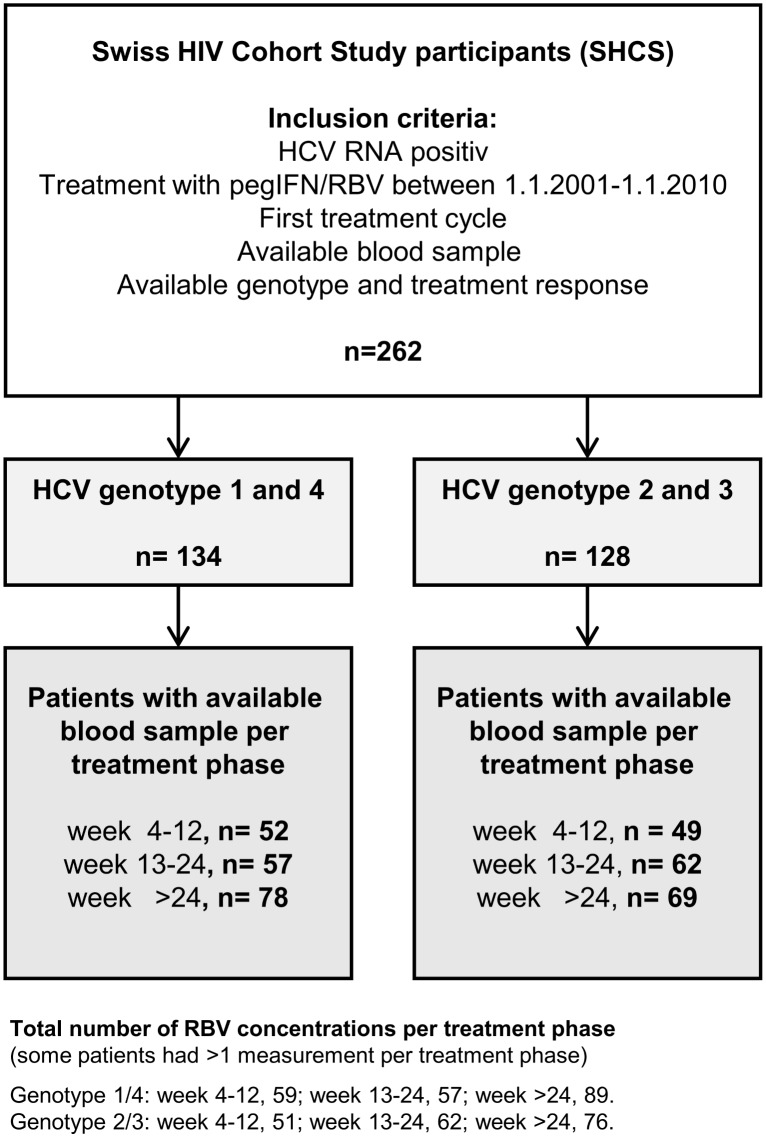
We included 262 HCV treatment naïve HIV/HCV-coinfected Swiss HIV Cohort Study (SHCS) participants treated with RBV and pegIFN between 01.01.2001-01.01.2010, 134 with HCV genotype (GT) 1/4, and 128 with GT 2/3 infections. RBV levels were measured retrospectively in stored plasma samples obtained between HCV treatment week 4 and end of therapy. Uni- and multivariable logistic regression analyses were used to evaluate the association between RBV concentration and SVR in GT 1/4 and GT 2/3 infections. The analyses were repeated stratified by treatment phase (week 4-12, 13-24, >24) and IL28B genotype (CC versus CT/TT).
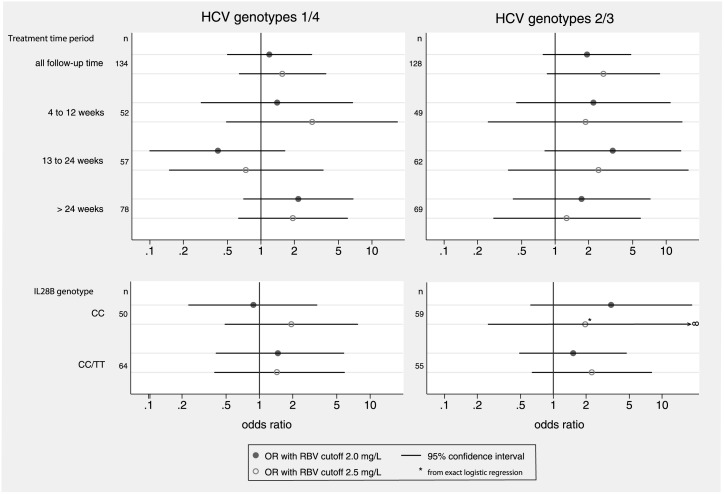
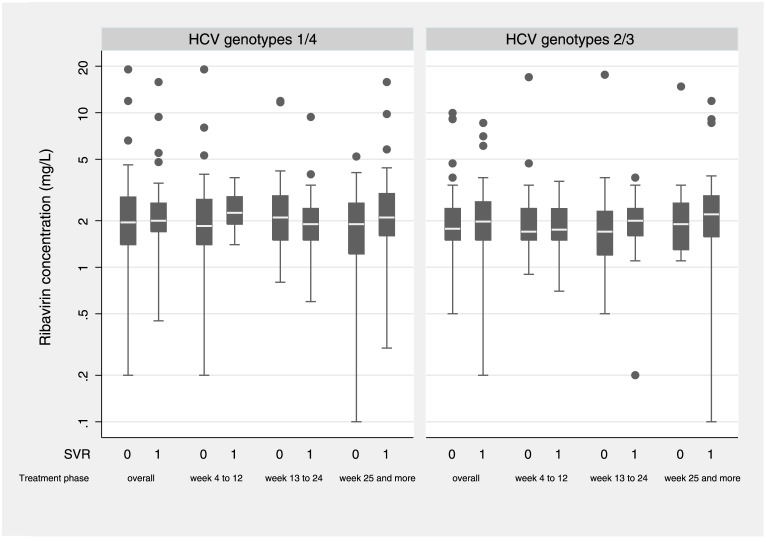
SVR rates were 35.1% in GT 1/4 and 70.3% in GT 2/3 infections. Overall, median RBV concentration was 2.0 mg/L in GT 1/4, and 1.9 mg/L in GT 2/3, and did not change significantly across treatment phases. Patients with SVR had similar RBV concentrations compared to patients without SVR in both HCV genotype groups. SVR was not associated with RBV levels ≥2.0 mg/L (GT 1/4, OR 1.19 [0.5-2.86]; GT 2/3, 1.94 [0.78-4.80]) and ≥2.5 mg/L (GT 1/4, 1.56 [0.64-3.84]; GT 2/3 2.72 [0.85-8.73]), regardless of treatment phase, and IL28B genotype.
In HIV/HCV-coinfected patients treated with pegIFN/RBV, therapeutic drug monitoring of RBV concentrations does not enhance the chance of HCV cure, regardless of HCV genotype, treatment phase and IL28B genotype.
利巴韦林(RBV)是当前大多数丙型肝炎(HCV)治疗方案的重要组成部分,在资源有限的环境中,与聚乙二醇化干扰素(pegIFN)联合用于治疗慢性HCV仍是标准治疗方法。关于RBV浓度与持续病毒学应答(SVR)之间是否相关,HIV/HCV合并感染患者的研究结果相互矛盾。
我们纳入了262例未经HCV治疗的HIV/HCV合并感染的瑞士HIV队列研究(SHCS)参与者,他们在2001年1月1日至2010年1月1日期间接受了RBV和pegIFN治疗,其中134例为HCV基因(GT)1/4型感染,128例为GT 2/3型感染。回顾性测量在HCV治疗第4周和治疗结束之间采集的储存血浆样本中的RBV水平。采用单变量和多变量逻辑回归分析来评估GT 1/4型和GT 2/3型感染中RBV浓度与SVR之间的关联。分析按治疗阶段(第4 - 12周、第13 - 24周、>24周)和IL28B基因型(CC与CT/TT)进行分层重复。
GT 1/4型感染的SVR率为35.1%,GT 2/3型感染的SVR率为70.3%。总体而言,GT 1/4型的RBV浓度中位数为2.0 mg/L,GT 2/3型为1.9 mg/L,且在各治疗阶段无显著变化。在两个HCV基因型组中,获得SVR的患者与未获得SVR的患者的RBV浓度相似。无论治疗阶段和IL28B基因型如何,SVR与RBV水平≥2.0 mg/L(GT 1/4型,比值比[OR]1.19[0.5 - 2.86];GT 2/3型,1.94[0.78 - 4.80])和≥2.5 mg/L(GT 1/4型,1.56[0.64 - 3.84];GT 2/3型,2.72[0.85 - 8.73])均无关联。
在接受pegIFN/RBV治疗的HIV/HCV合并感染患者中,无论HCV基因型、治疗阶段和IL28B基因型如何,对RBV浓度进行治疗药物监测均不能提高HCV治愈的机会。