Haverkamp Leonie, Brenkman Hylke J F, Seesing Maarten F J, Gisbertz Suzanne S, van Berge Henegouwen Mark I, Luyer Misha D P, Nieuwenhuijzen Grard A P, Wijnhoven Bas P L, van Lanschot Jan J B, de Steur Wobbe O, Hartgrink Henk H, Stoot Jan H M B, Hulsewé Karel W E, Spillenaar Bilgen Ernst J, Rütter Jeroen E, Kouwenhoven Ewout A, van Det Marc J, van der Peet Donald L, Daams Freek, Draaisma Werner A, Broeders Ivo A M J, van Stel Henk F, Lacle Miangela M, Ruurda Jelle P, van Hillegersberg Richard
University Medical Center Utrecht, Heidelberglaan 100, 3584 CX, Utrecht, The Netherlands.
Academic Medical Center, Meibergdreef 9, 1105 AZ, Amsterdam, The Netherlands.
BMC Cancer. 2015 Jul 29;15:556. doi: 10.1186/s12885-015-1551-z.
For gastric cancer patients, surgical resection with en-bloc lymphadenectomy is the cornerstone of curative treatment. Open gastrectomy has long been the preferred surgical approach worldwide. However, this procedure is associated with considerable morbidity. Several meta-analyses have shown an advantage in short-term outcomes of laparoscopic gastrectomy compared to open procedures, with similar oncologic outcomes. However, it remains unclear whether the results of these Asian studies can be extrapolated to the Western population. In this trial from the Netherlands, patients with resectable gastric cancer will be randomized to laparoscopic or open gastrectomy.
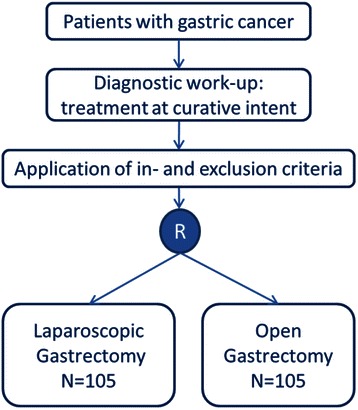
The study is a non-blinded, multicenter, prospectively randomized controlled superiority trial. Patients (≥18 years) with histologically proven, surgically resectable (cT1-4a, N0-3b, M0) gastric adenocarcinoma and European Clinical Oncology Group performance status 0, 1 or 2 are eligible to participate in the study after obtaining informed consent. Patients (n = 210) will be included in one of the ten participating Dutch centers and are randomized to either laparoscopic or open gastrectomy. The primary outcome is postoperative hospital stay (days). Secondary outcome parameters include postoperative morbidity and mortality, oncologic outcomes, readmissions, quality of life and cost-effectiveness.
In this randomized controlled trial laparoscopic and open gastrectomy are compared in patients with resectable gastric cancer. It is expected that laparoscopic gastrectomy will result in a faster recovery of the patient and a shorter hospital stay. Secondly, it is expected that laparoscopic gastrectomy will be associated with a lower postoperative morbidity, less readmissions, higher cost-effectiveness, better postoperative quality of life, but with similar mortality and oncologic outcomes, compared to open gastrectomy. The study started on 1 December 2014. Inclusion and follow-up will take 3 and 5 years respectively. Short-term results will be analyzed and published after discharge of the last randomized patient.
NCT02248519.
对于胃癌患者,整块淋巴结清扫的手术切除是根治性治疗的基石。开放胃切除术长期以来一直是全球首选的手术方式。然而,该手术伴随着相当高的发病率。多项荟萃分析表明,与开放手术相比,腹腔镜胃切除术在短期结局方面具有优势,肿瘤学结局相似。然而,这些亚洲研究的结果是否能外推至西方人群仍不明确。在这项来自荷兰的试验中,可切除胃癌患者将被随机分配接受腹腔镜或开放胃切除术。
本研究是一项非盲、多中心、前瞻性随机对照优势试验。经组织学证实、手术可切除(cT1 - 4a,N0 - 3b,M0)的胃腺癌患者,且欧洲临床肿瘤学会体能状态为0、1或2,在获得知情同意后有资格参与本研究。患者(n = 210)将被纳入荷兰十个参与中心之一,并随机分配接受腹腔镜或开放胃切除术。主要结局是术后住院天数。次要结局参数包括术后发病率和死亡率、肿瘤学结局、再入院情况、生活质量和成本效益。
在这项随机对照试验中,对可切除胃癌患者的腹腔镜和开放胃切除术进行了比较。预计腹腔镜胃切除术将使患者恢复更快、住院时间更短。其次,预计与开放胃切除术相比,腹腔镜胃切除术术后发病率更低、再入院次数更少、成本效益更高、术后生活质量更好,但死亡率和肿瘤学结局相似。该研究于2014年12月1日开始。纳入和随访将分别持续3年和5年。最后一名随机分组患者出院后将分析并发表短期结果。
NCT02248519