Department of Surgery, University Medical Center (UMC) Utrecht, G04.228, 3508 GA, Utrecht, The Netherlands.
Department of Pathology, University Medical Center Utrecht, Utrecht, The Netherlands.
J Gastrointest Surg. 2023 Sep;27(9):1812-1824. doi: 10.1007/s11605-023-05683-z. Epub 2023 Jun 20.
Distal gastrectomy (DG) for gastric cancer can cause less morbidity than total gastrectomy (TG), but may compromise radicality. No prospective studies administered neoadjuvant chemotherapy, and few assessed quality of life (QoL).
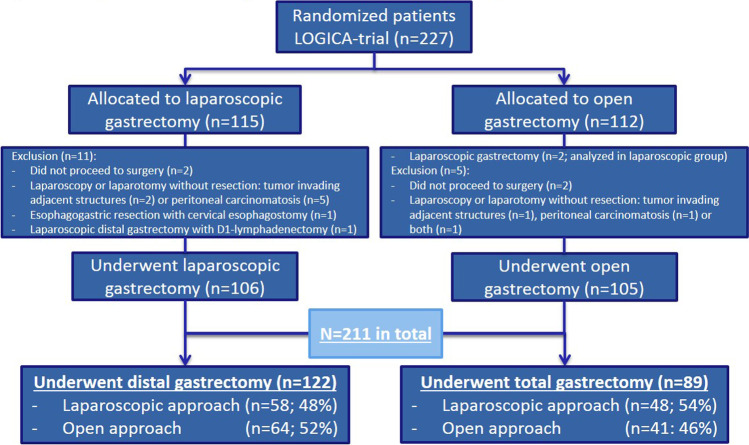
The multicenter LOGICA-trial randomized laparoscopic versus open D2-gastrectomy for resectable gastric adenocarcinoma (cT1-4aN0-3bM0) in 10 Dutch hospitals. This secondary LOGICA-analysis compared surgical and oncological outcomes after DG versus TG. DG was performed for non-proximal tumors if R0-resection was deemed achievable, TG for other tumors. Postoperative complications, mortality, hospitalization, radicality, nodal yield, 1-year survival, and EORTC-QoL-questionnaires were analyzed using Χ-/Fisher's exact tests and regression analyses.
Between 2015 and 2018, 211 patients underwent DG (n = 122) or TG (n = 89), and 75% of patients underwent neoadjuvant chemotherapy. DG-patients were older, had more comorbidities, less diffuse type tumors, and lower cT-stage than TG-patients (p < 0.05). DG-patients experienced fewer overall complications (34% versus 57%; p < 0.001), also after correcting for baseline differences, lower anastomotic leakage (3% versus 19%), pneumonia (4% versus 22%), atrial fibrillation (3% versus 14%), and Clavien-Dindo grading compared to TG-patients (p < 0.05), and demonstrated shorter median hospital stay (6 versus 8 days; p < 0.001). QoL was better after DG (statistically significant and clinically relevant) in most 1-year postoperative time points. DG-patients showed 98% R0-resections, and similar 30-/90-day mortality, nodal yield (28 versus 30 nodes; p = 0.490), and 1-year survival after correcting for baseline differences (p = 0.084) compared to TG-patients.
If oncologically feasible, DG should be preferred over TG due to less complications, faster postoperative recovery, and better QoL while achieving equivalent oncological effectiveness. Distal D2-gastrectomy for gastric cancer resulted in less complications, shorter hospitalization, quicker recovery and better quality of life compared to total D2-gastrectomy, whereas radicality, nodal yield and survival were similar.
与全胃切除术(TG)相比,远端胃切除术(DG)治疗胃癌的发病率较低,但可能会影响根治性。没有前瞻性研究进行新辅助化疗,很少评估生活质量(QoL)。
这项多中心 LOGICA 试验在荷兰的 10 家医院中,对可切除的胃腺癌(cT1-4aN0-3bM0)患者进行了腹腔镜与开放的 D2 胃切除术的随机对照试验。该二次 LOGICA 分析比较了 DG 与 TG 后的手术和肿瘤学结果。如果认为可以实现 R0 切除,则对非近端肿瘤进行 DG,如果为其他肿瘤,则进行 TG。使用 Χ-/Fisher 精确检验和回归分析分析术后并发症、死亡率、住院时间、根治性、淋巴结产量、1 年生存率和 EORTC-QoL 问卷。
2015 年至 2018 年间,211 例患者接受了 DG(n=122)或 TG(n=89)治疗,其中 75%的患者接受了新辅助化疗。DG 患者比 TG 患者年龄更大,合并症更多,弥漫性肿瘤更少,cT 分期更低(p<0.05)。DG 患者总体并发症发生率较低(34%对 57%;p<0.001),即使校正了基线差异后,吻合口漏(3%对 19%)、肺炎(4%对 22%)、心房颤动(3%对 14%)和 Clavien-Dindo 分级也较低(p<0.05),并且中位住院时间较短(6 天对 8 天;p<0.001)。在大多数 1 年术后时间点,DG 后 QoL 更好(具有统计学意义和临床相关性)。DG 患者 98%实现了 R0 切除,30/90 天死亡率、淋巴结产量(28 个对 30 个淋巴结;p=0.490)和校正基线差异后的 1 年生存率(p=0.084)与 TG 患者相似。
如果在肿瘤学上可行,DG 应优先于 TG,因为 DG 并发症更少,术后恢复更快,QoL 更好,而肿瘤学效果相当。与全胃切除术(TG)相比,远端胃切除术(DG)治疗胃癌的并发症更少,住院时间更短,恢复更快,生活质量更高,而根治性、淋巴结产量和生存率相似。