Rincon Melvin Y, VandenDriessche Thierry, Chuah Marinee K
Department of Gene Therapy and Regenerative Medicine, Free University of Brussels (VUB), Building D, room D306, Laarbeeklaan 103, Brussels, Belgium Centro de Investigaciones, Fundacion Cardiovascular de Colombia, Floridablanca, Colombia.
Department of Gene Therapy and Regenerative Medicine, Free University of Brussels (VUB), Building D, room D306, Laarbeeklaan 103, Brussels, Belgium Center for Molecular and Vascular Biology, Department of Cardiovascular Sciences, University of Leuven, Leuven, Belgium
Cardiovasc Res. 2015 Oct 1;108(1):4-20. doi: 10.1093/cvr/cvv205. Epub 2015 Aug 3.
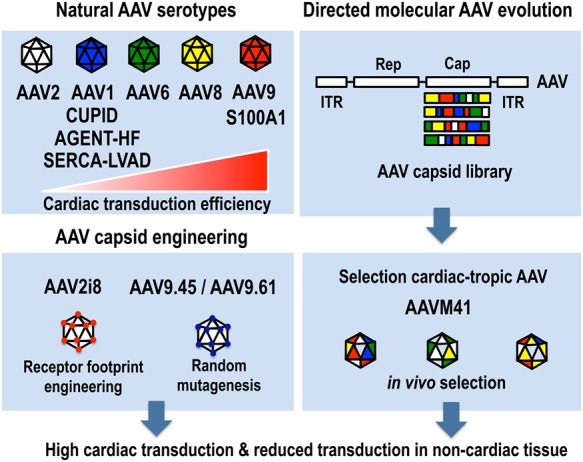
Gene therapy is a promising modality for the treatment of inherited and acquired cardiovascular diseases. The identification of the molecular pathways involved in the pathophysiology of heart failure and other associated cardiac diseases led to encouraging preclinical gene therapy studies in small and large animal models. However, the initial clinical results yielded only modest or no improvement in clinical endpoints. The presence of neutralizing antibodies and cellular immune responses directed against the viral vector and/or the gene-modified cells, the insufficient gene expression levels, and the limited gene transduction efficiencies accounted for the overall limited clinical improvements. Nevertheless, further improvements of the gene delivery technology and a better understanding of the underlying biology fostered renewed interest in gene therapy for heart failure. In particular, improved vectors based on emerging cardiotropic serotypes of the adeno-associated viral vector (AAV) are particularly well suited to coax expression of therapeutic genes in the heart. This led to new clinical trials based on the delivery of the sarcoplasmic reticulum Ca(2+)-ATPase protein (SERCA2a). Though the first clinical results were encouraging, a recent Phase IIb trial did not confirm the beneficial clinical outcomes that were initially reported. New approaches based on S100A1 and adenylate cyclase 6 are also being considered for clinical applications. Emerging paradigms based on the use of miRNA regulation or CRISPR/Cas9-based genome engineering open new therapeutic perspectives for treating cardiovascular diseases by gene therapy. Nevertheless, the continuous improvement of cardiac gene delivery is needed to allow the use of safer and more effective vector doses, ultimately bringing gene therapy for heart failure one step closer to reality.
基因治疗是治疗遗传性和获得性心血管疾病的一种有前景的方法。对心力衰竭和其他相关心脏疾病病理生理学中涉及的分子途径的鉴定,在小型和大型动物模型中引发了令人鼓舞的临床前基因治疗研究。然而,最初的临床结果在临床终点方面仅产生了适度的改善或没有改善。针对病毒载体和/或基因修饰细胞的中和抗体和细胞免疫反应的存在、基因表达水平不足以及基因转导效率有限,导致了整体有限的临床改善。尽管如此,基因递送技术的进一步改进以及对基础生物学的更好理解,重新激发了人们对心力衰竭基因治疗的兴趣。特别是,基于腺相关病毒载体(AAV)新出现的嗜心性血清型的改进载体特别适合在心脏中诱导治疗性基因的表达。这导致了基于肌浆网Ca(2+)-ATP酶蛋白(SERCA2a)递送的新临床试验。尽管最初的临床结果令人鼓舞,但最近的一项IIb期试验并未证实最初报道的有益临床结果。基于S100A1和腺苷酸环化酶6的新方法也正在考虑用于临床应用。基于使用miRNA调节或CRISPR/Cas9基因组工程的新兴模式为通过基因治疗治疗心血管疾病开辟了新的治疗前景。尽管如此,仍需要不断改进心脏基因递送,以便能够使用更安全、更有效的载体剂量,最终使心力衰竭的基因治疗更接近现实。