Capatina Cristina, Paluzzi Alessandro, Mitchell Rosalid, Karavitaki Niki
Carol Davila University of Medicine and Pharmacy, Endocrinology Department, 34-36 Aviatorilor Blvd, Bucharest 050474, Romania.
Neurosurgery, University Hospitals Birmingham NHS Foundation Trust, Queen Elizabeth Hospital, Birmingham, B15 2TH, UK.
J Clin Med. 2015 Jul 13;4(7):1448-62. doi: 10.3390/jcm4071448.
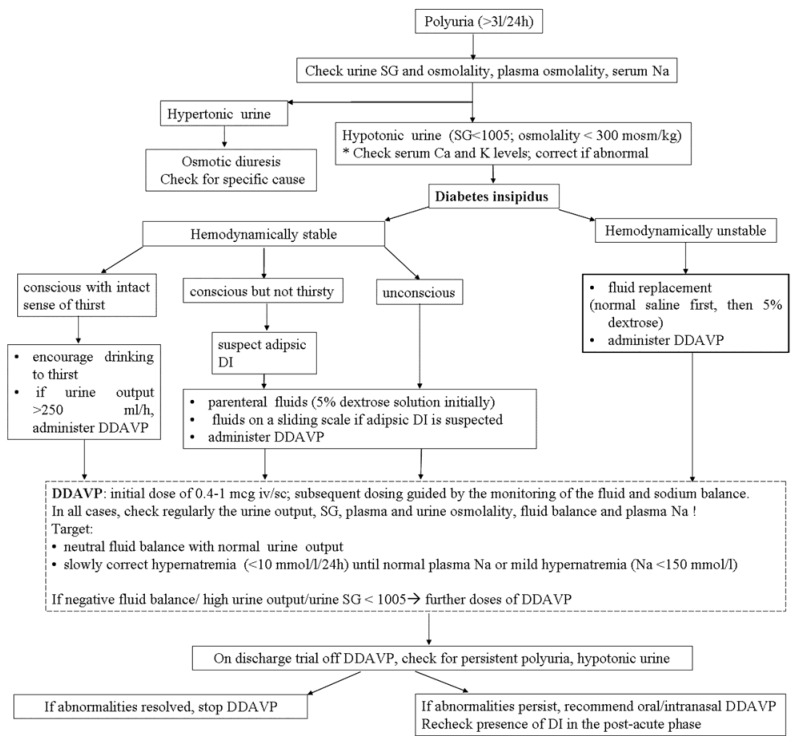
Traumatic brain injury (TBI) is a significant cause of morbidity and mortality in many age groups. Neuroendocrine dysfunction has been recognized as a consequence of TBI and consists of both anterior and posterior pituitary insufficiency; water and electrolyte abnormalities (diabetes insipidus (DI) and the syndrome of inappropriate antidiuretic hormone secretion (SIADH)) are amongst the most challenging sequelae. The acute head trauma can lead (directly or indirectly) to dysfunction of the hypothalamic neurons secreting antidiuretic hormone (ADH) or of the posterior pituitary gland causing post-traumatic DI (PTDI). PTDI is usually diagnosed in the first days after the trauma presenting with hypotonic polyuria. Frequently, the poor general status of most patients prevents adequate fluid intake to compensate the losses and severe dehydration and hypernatremia occur. Management consists of careful monitoring of fluid balance and hormonal replacement. PTDI is associated with high mortality, particularly when presenting very early following the injury. In many surviving patients, the PTDI is transient, lasting a few days to a few weeks and in a minority of cases, it is permanent requiring management similar to that offered to patients with non-traumatic central DI.
创伤性脑损伤(TBI)是许多年龄组发病和死亡的重要原因。神经内分泌功能障碍已被认为是TBI的后果,包括垂体前叶和后叶功能不全;水和电解质异常(尿崩症(DI)和抗利尿激素分泌不当综合征(SIADH))是最具挑战性的后遗症之一。急性头部创伤可(直接或间接)导致分泌抗利尿激素(ADH)的下丘脑神经元或垂体后叶功能障碍,从而引起创伤后尿崩症(PTDI)。PTDI通常在创伤后的头几天被诊断出来,表现为低渗性多尿。通常,大多数患者的一般状况较差,无法摄入足够的液体来补偿损失,从而发生严重脱水和高钠血症。治疗包括仔细监测液体平衡和激素替代。PTDI与高死亡率相关,尤其是在受伤后很早就出现时。在许多存活的患者中,PTDI是短暂的,持续几天到几周,在少数情况下,它是永久性的,需要与非创伤性中枢性尿崩症患者相似的治疗。