Al Halabi Shadi, Qintar Mohammed, Hussein Ayman, Alraies M Chadi, Jones David G, Wong Tom, MacDonald Michael R, Petrie Mark C, Cantillon Daniel, Tarakji Khaldoun G, Kanj Mohamed, Bhargava Mandeep, Varma Niraj, Baranowski Bryan, Wilkoff Bruce L, Wazni Oussama, Callahan Thomas, Saliba Walid, Chung Mina K
The Department of Cardiovascular Medicine, Heart & Vascular Institute, Cleveland Clinic, Cleveland, OH.
The Department of Cardiology, University of Minnesota, Minneapolis, MN.
JACC Clin Electrophysiol. 2015 Jun 1;1(3):200-209. doi: 10.1016/j.jacep.2015.02.018.
Rhythm control with antiarrhythmic drugs (AADs) is not superior to rate control in patients with heart failure (HF) and atrial fibrillation (AF), but AF ablation may be more successful at achieving rhythm control than AADs. However, risks for both ablation and AADs are likely higher and success rates lower in patients with HF.
To compare rate control versus AF catheter ablation strategies in patients with AF and HF.
We conducted a meta-analysis of trials which randomized HF patients (LVEF<50%) with AF to a rate control or AF catheter ablation strategy and reported change in LVEF, quality of life, 6-minute walk test, or peak oxygen consumption. Study quality and heterogenity were assessed using Jadad scores and Cochran's Q statistics, respectively. Mantel Haenszel relative risks and mean differences were calculated using random effect models.
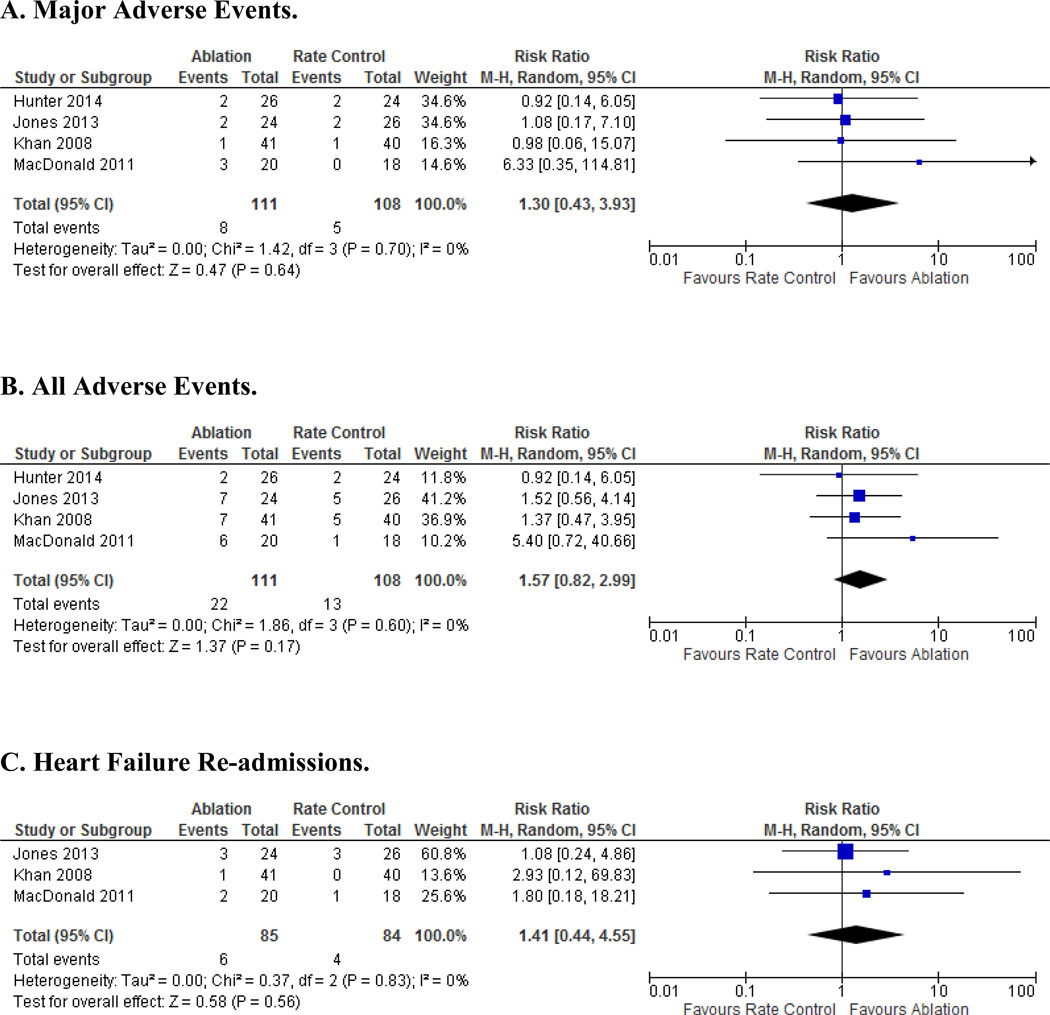
Four trials (N=224) met inclusion criteria; 82.5% (n=185) had persistent AF. AF ablation was associated with an increase in LVEF (mean difference 8.5%; 95%CI 6.4,10.7%; P<0.001) compared to rate control. AF ablation was superior in improving quality of life by Minnesota Living with Heart Failure (MLWHF) questionnaire scores (mean difference -11.9; 95%CI -17.1, -6.6; P<0.001). Peak oxygen consumption and 6-minute walk distance increased in AF ablation compared to rate control patients (mean difference 3.2; 95%CI 1.1,5.2; P=0.003; mean difference 34.8; 95%CI 2.9, 66.7; P = 0.03, respectively). In the persistent AF subgroup LVEF and MLWHF were significantly improved with AF ablation. Major adverse event rates (RR 1.3; 95% CI, 0.4, 3.9; p=0.64) were not significantly different. No significant heterogeneity was evident.
In patients with HF and AF, AF catheter ablation is superior to rate control in improving LVEF, quality of life and functional capacity. Prior to accepting a rate control strategy in HF patients with persistent or drug refractory AF, consideration should be given to AF ablation.
在心力衰竭(HF)合并心房颤动(AF)的患者中,使用抗心律失常药物(AADs)进行节律控制并不优于心率控制,但AF消融在实现节律控制方面可能比AADs更成功。然而,HF患者进行消融和使用AADs的风险可能更高,成功率更低。
比较AF和HF患者的心率控制与AF导管消融策略。
我们对将AF合并HF患者(左心室射血分数[LVEF]<50%)随机分为心率控制或AF导管消融策略的试验进行了荟萃分析,并报告了LVEF、生活质量、6分钟步行试验或峰值耗氧量的变化。分别使用Jadad评分和Cochran Q统计量评估研究质量和异质性。使用随机效应模型计算Mantel Haenszel相对风险和平均差异。
四项试验(N = 224)符合纳入标准;82.5%(n = 185)为持续性AF。与心率控制相比,AF消融与LVEF增加相关(平均差异8.5%;95%CI 6.4,10.7%;P<0.001)。通过明尼苏达心力衰竭生活问卷(MLWHF)评分,AF消融在改善生活质量方面更优(平均差异-11.9;95%CI -17.1,-6.6;P<0.001)。与心率控制患者相比,AF消融患者的峰值耗氧量和6分钟步行距离增加(平均差异3.