Luo Miao, Zheng Hai-Yan, Zhang Ying, Feng Yuan, Li Dan-Qing, Li Xiao-Lin, Han Jian-Fang, Li Tao-Ping
Sleep Disorder Center, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong 510515, China.
Chin Med J (Engl). 2015 Aug 20;128(16):2134-40. doi: 10.4103/0366-6999.162514.
The currently available polysomnography (PSG) equipments and operating personnel are facing increasing pressure, such situation may result in the problem that a large number of obstructive sleep apnea (OSA) patients cannot receive timely diagnosis and treatment, we sought to develop a nomogram quantifying the risk of OSA for a better decision of using PSG, based on the clinical syndromes and the demographic and anthropometric characteristics.
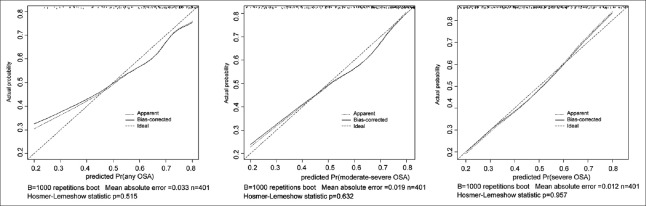
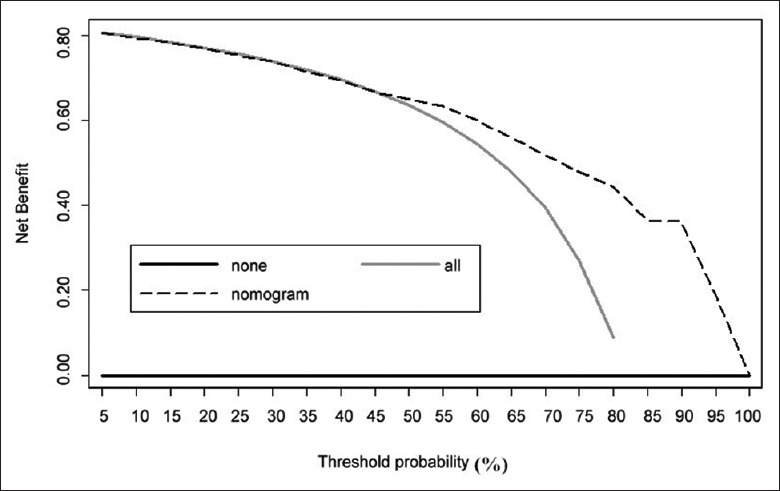
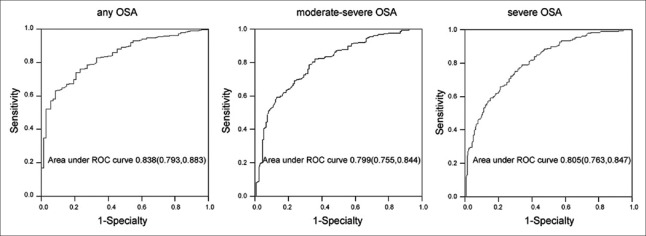
The nomogram was constructed through an ordinal logistic regression procedure. Predictive accuracy and performance characteristics were assessed with the area under the curve (AUC) of the receiver operating characteristics and calibration plots, respectively. Decision curve analyses were applied to assess the net benefit of the nomogram.
Among the 401 patients, 73 (18.2%) were diagnosed and grouped as the none OSA (apnea-hypopnea index [AHI] <5), 67 (16.7%) the mild OSA (5 ≤ AHI < 15), 82 (20.4%) the moderate OSA (15 ≤ AHI < 30), and 179 (44.6%) the severe OSA (AHI ≥ 30). The multivariable analysis suggested the significant factors were duration of disease, smoking status, difficulty of falling asleep, lack of energy, and waist circumference. A nomogram was created for the prediction of OSA using these clinical parameters and was internally validated using bootstrapping method. The discrimination accuracies of the nomogram for any OSA, moderate-severe OSA, and severe OSA were 83.8%, 79.9%, and 80.5%, respectively, which indicated good calibration. Decision curve analysis showed that using nomogram could reduce the unnecessary polysomnography (PSG) by 10% without increasing the false negatives.
The established clinical nomogram provides high accuracy in predicting the individual risk of OSA. This tool may help physicians better make decisions on PSG arrangement for the patients referred to sleep centers.
目前可用的多导睡眠监测(PSG)设备和操作人员面临着越来越大的压力,这种情况可能导致大量阻塞性睡眠呼吸暂停(OSA)患者无法得到及时诊断和治疗,我们试图基于临床症状、人口统计学和人体测量学特征开发一种列线图,以量化OSA风险,从而更好地决定是否使用PSG。
通过有序逻辑回归程序构建列线图。分别使用受试者工作特征曲线下面积(AUC)和校准图评估预测准确性和性能特征。应用决策曲线分析评估列线图的净效益。
在401例患者中,73例(18.2%)被诊断为非OSA(呼吸暂停低通气指数[AHI]<5),67例(16.7%)为轻度OSA(5≤AHI<15),82例(20.4%)为中度OSA(15≤AHI<30),179例(44.6%)为重度OSA(AHI≥30)。多变量分析表明,显著因素为病程、吸烟状况、入睡困难、精力不足和腰围。使用这些临床参数创建了一个用于预测OSA的列线图,并使用自举法进行内部验证。该列线图对任何OSA、中重度OSA和重度OSA的鉴别准确率分别为83.8%、79.9%和80.5%,表明校准良好。决策曲线分析表明,使用列线图可减少10%的不必要多导睡眠监测(PSG),而不会增加假阴性。
所建立的临床列线图在预测个体OSA风险方面具有较高的准确性。该工具可能有助于医生更好地为转诊至睡眠中心的患者做出PSG安排决策。