Reifschneider Kent, Auble Bethany A, Rose Susan R
Children's Hospital of The Kings Daughters, Eastern Virginia Medical School, Norfolk, Virginia, VA 23507, USA.
Children's Hospital of Wisconsin, Medical College of Wisconsin, Milwaukee, Wisconsin, WI 53226, USA.
J Clin Med. 2015 Jul 31;4(8):1536-60. doi: 10.3390/jcm4081536.
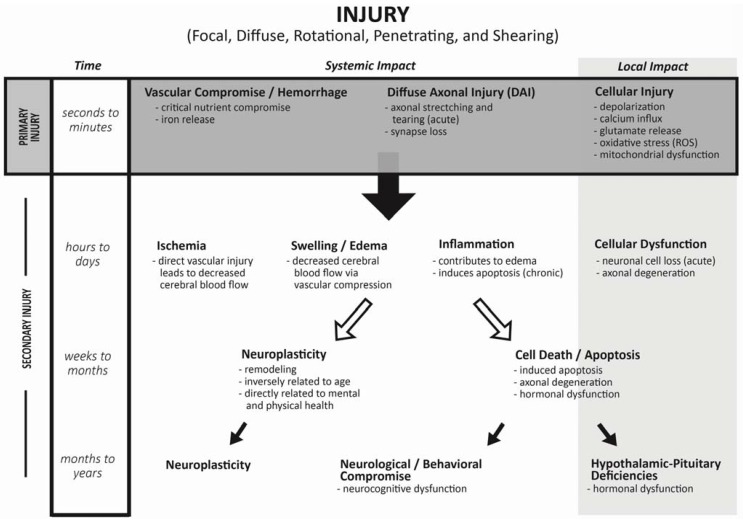
Traumatic brain injuries (TBI) are common occurrences in childhood, often resulting in long term, life altering consequences. Research into endocrine sequelae following injury has gained attention; however, there are few studies in children. This paper reviews the pathophysiology and current literature documenting risk for endocrine dysfunction in children suffering from TBI. Primary injury following TBI often results in disruption of the hypothalamic-pituitary-adrenal axis and antidiuretic hormone production and release, with implications for both acute management and survival. Secondary injuries, occurring hours to weeks after TBI, result in both temporary and permanent alterations in pituitary function. At five years after moderate to severe TBI, nearly 30% of children suffer from hypopituitarism. Growth hormone deficiency and disturbances in puberty are the most common; however, any part of the hypothalamic-pituitary axis can be affected. In addition, endocrine abnormalities can improve or worsen with time, having a significant impact on children's quality of life both acutely and chronically. Since primary and secondary injuries from TBI commonly result in transient or permanent hypopituitarism, we conclude that survivors should undergo serial screening for possible endocrine disturbances. High indices of suspicion for life threatening endocrine deficiencies should be maintained during acute care. Additionally, survivors of TBI should undergo endocrine surveillance by 6-12 months after injury, and then yearly, to ensure early detection of deficiencies in hormonal production that can substantially influence growth, puberty and quality of life.
创伤性脑损伤(TBI)在儿童时期很常见,常常会导致长期的、改变生活的后果。对损伤后内分泌后遗症的研究已受到关注;然而,针对儿童的研究却很少。本文综述了TBI患儿内分泌功能障碍的病理生理学及记录其风险的当前文献。TBI后的原发性损伤常导致下丘脑 - 垂体 - 肾上腺轴以及抗利尿激素的产生和释放受到破坏,这对急性处理和生存都有影响。继发性损伤发生在TBI后的数小时至数周内,会导致垂体功能出现暂时和永久性改变。在中度至重度TBI发生五年后,近30%的儿童患有垂体功能减退症。生长激素缺乏和青春期紊乱最为常见;然而,下丘脑 - 垂体轴的任何部分都可能受到影响。此外,内分泌异常会随时间改善或恶化,对儿童的急性和慢性生活质量都有重大影响。由于TBI的原发性和继发性损伤通常会导致短暂或永久性垂体功能减退,我们得出结论,幸存者应接受系列筛查以排查可能的内分泌紊乱。在急性护理期间,应高度怀疑存在危及生命的内分泌缺乏症。此外,TBI幸存者应在受伤后6 - 12个月接受内分泌监测,之后每年监测一次,以确保早期发现可能严重影响生长、青春期和生活质量的激素分泌不足。