Wei Wen-Cheng, Wu Ching-Yang, Wu Ching-Feng, Fu Jui-Ying, Su Ta-Wei, Yu Sheng-Yueh, Kao Tsung-Chi, Ko Po-Jen
From the Department of Surgery, Division of Thoracic and Cardiovascular Surgery (W-CW, C-YW, C-FW, T-WS, S-YY, T-CK, P-JK); and Department of Internal Medicine, Division of Chest and Critical Care, Chang Gung Memorial Hospital, Chang Gung University, Taoyuan, Taiwan (J-YF).
Medicine (Baltimore). 2015 Aug;94(33):e1381. doi: 10.1097/MD.0000000000001381.
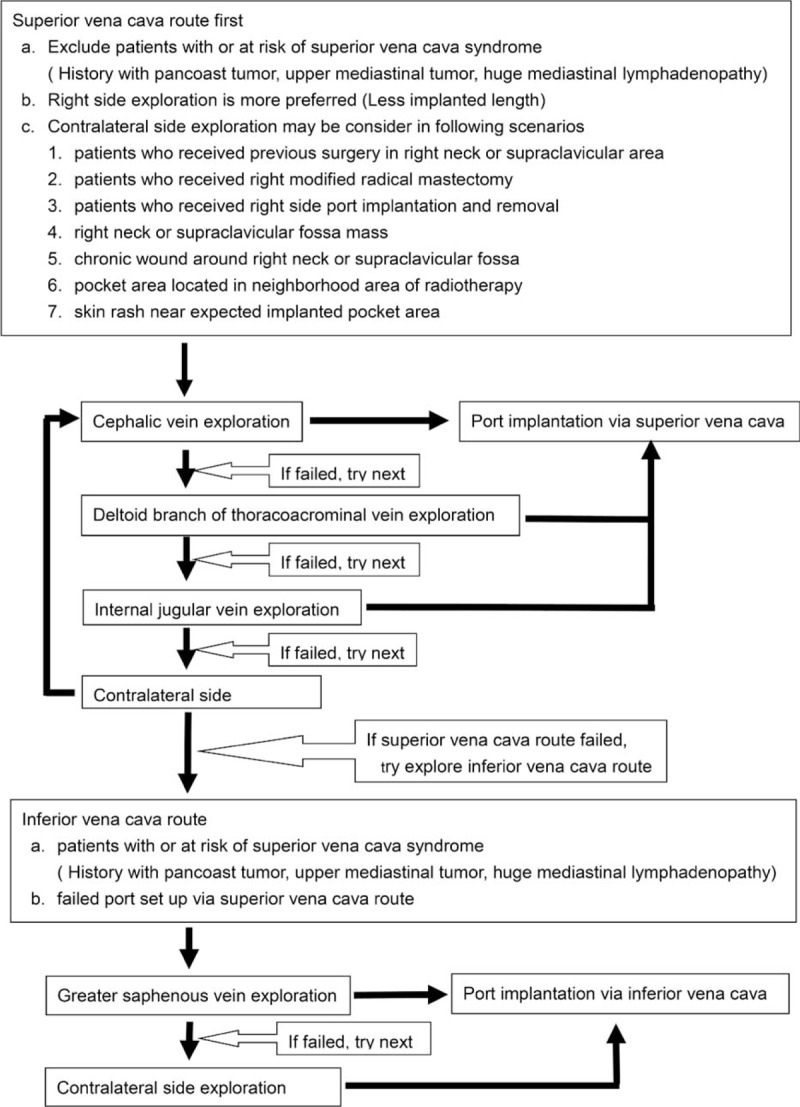
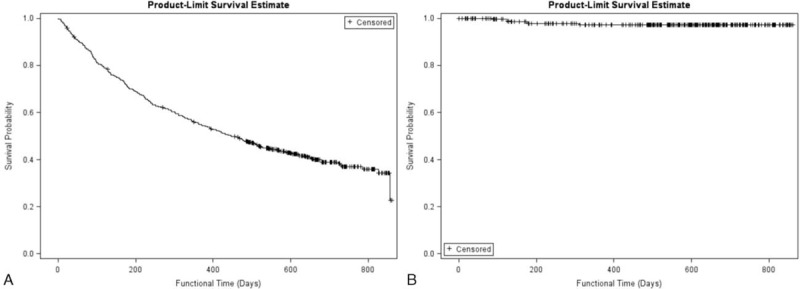
Vascular cutdown and echo guide puncture methods have its own limitations under certain conditions. There was no available algorithm for choosing entry vessel. A standard algorithm was introduced to help choose the entry vessel location according to our clinical experience and review of the literature. The goal of this study is to analyze the treatment results of the standard algorithm used to choose the entry vessel for intravenous port implantation.During the period between March 2012 and March 2013, 507 patients who received intravenous port implantation due to advanced chemotherapy were included into this study. Choice of entry vessel was according to standard algorithm. All clinical characteristic factors were collected and complication rate and incidence were further analyzed.Compared with our clinical experience in 2006, procedure-related complication rate declined from 1.09% to 0.4%, whereas the late complication rate decreased from 19.97% to 3.55%. No more pneumothorax, hematoma, catheter kinking, fractures, and pocket erosion were identified after using the standard algorithm. In alive oncology patients, 98% implanted port could serve a functional vascular access to fit therapeutic needs.This standard algorithm for choosing the best entry vessel is a simple guideline that is easy to follow. The algorithm has excellent efficiency and can minimize complication rates and incidence.
在某些情况下,血管切开术和超声引导穿刺方法有其自身的局限性。目前尚无选择入路血管的可用算法。根据我们的临床经验和文献回顾,引入了一种标准算法来帮助选择入路血管位置。本研究的目的是分析用于选择静脉输液港植入入路血管的标准算法的治疗效果。
在2012年3月至2013年3月期间,本研究纳入了507例因晚期化疗而接受静脉输液港植入的患者。入路血管的选择依据标准算法。收集所有临床特征因素,并进一步分析并发症发生率。
与我们2006年的临床经验相比,手术相关并发症发生率从1.09%降至0.4%,而晚期并发症发生率从19.97%降至3.55%。使用标准算法后,未再出现气胸、血肿、导管扭结、断裂和囊袋侵蚀等情况。在存活的肿瘤患者中,98%的植入输液港能够提供符合治疗需求的功能性血管通路。
这种选择最佳入路血管的标准算法是一种易于遵循的简单指南。该算法效率极高,能够将并发症发生率降至最低。