Shen Te-Chun, Wang I-Kuan, Wei Chang-Ching, Lin Cheng-Li, Tsai Chia-Ta, Hsia Te-Chun, Sung Fung-Chang, Kao Chia-Hung
From Graduate Institute of Clinical Medicine Science, College of Medicine, China Medical University, Taichung, Taiwan (T-CS, I-KW, C-TT, F-CS, C-HK); Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan (T-CS, T-CH); Intensive Care Unit, Chu Shang Show Chwan Hospital, Nantou, Taiwan (T-CS); Division of Nephrology, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan (I-KW); Division of Nephrology, Department of Pediatrics, China Medical University Hospital, Taichung, Taiwan (C-CW); Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan (C-LL, F-CS); Division of Infection, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan (C-TT); and Department of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan (C-HK).
Medicine (Baltimore). 2015 Aug;94(34):e1437. doi: 10.1097/MD.0000000000001437.
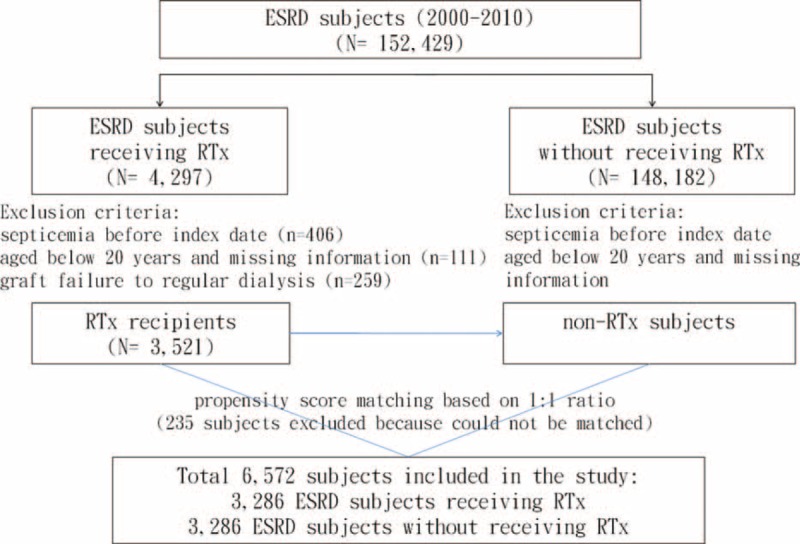
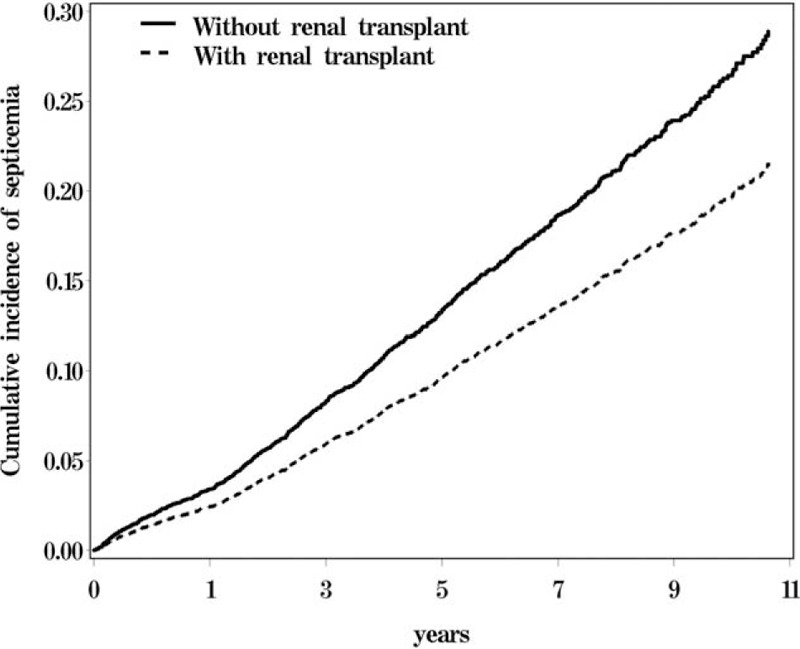
End-stage renal disease (ESRD) is a well-known risk factor for septicemia. Renal transplantation (RTx) is the treatment of choice for ESRD. However, RTx recipients should undergo long-term immunosuppressive therapy. The aim of this study was to evaluate the risk of septicemia in ESRD patients with and without RTx.This cohort study used the National Health Insurance (NHI) data of Taiwan from 2000 to 2010. The RTx group consisted of 3286 RTx recipients. The non-RTx comparison group also consisted of 3286 subjects with ESRD matched by propensity scores for age, sex, index date, comorbidities, and medications. The subjects were followed until the end of 2011 to evaluate the septicemia risk.The risk of septicemia was lower in the RTx group than the non-RTx group, with an adjusted hazard ratio of 0.73 [95% confidence interval (CI) = 0.64-0.84, P < 0.001]. In addition, we observed insignificantly lower intensive care unit (ICU) admission rate (35.8% vs. 39.8%) and lower 30-day all-cause mortality rate (17.2% vs. 18.5%) in the RTx group than the non-RTx group. However, the mean cost for septicemia in the RTx group was insignificantly higher than the non-RTx group (7175 vs. 6421 USD, P = 0.39).RTx recipients had a significantly reduced risk of developing septicemia compared to the propensity-matched non-RTx ESRD patients. The ICU admission and 30-day all-cause mortality rates also slightly decreased in RTx recipients but without statistical significance.
终末期肾病(ESRD)是败血症的一个众所周知的危险因素。肾移植(RTx)是ESRD的首选治疗方法。然而,肾移植受者应接受长期免疫抑制治疗。本研究的目的是评估接受和未接受肾移植的ESRD患者发生败血症的风险。
这项队列研究使用了台湾2000年至2010年的国民健康保险(NHI)数据。肾移植组由3286名肾移植受者组成。非肾移植对照组也由3286名ESRD受试者组成,这些受试者根据年龄、性别、索引日期、合并症和药物的倾向得分进行匹配。对受试者进行随访直至2011年底,以评估败血症风险。
肾移植组败血症风险低于非肾移植组,调整后的风险比为0.73[95%置信区间(CI)=0.64-0.84,P<0.001]。此外,我们观察到肾移植组的重症监护病房(ICU)入院率略低于非肾移植组(35.8%对39.8%),30天全因死亡率也略低于非肾移植组(17.2%对18.5%)。然而,肾移植组败血症的平均费用略高于非肾移植组(7175美元对6421美元,P=0.39)。
与倾向匹配的非肾移植ESRD患者相比,肾移植受者发生败血症的风险显著降低。肾移植受者的ICU入院率和30天全因死亡率也略有下降,但无统计学意义。