Shelton Jennifer M G, Corran Patrick, Risley Paul, Silva Nilupa, Hubbart Christina, Jeffreys Anna, Rowlands Kate, Craik Rachel, Cornelius Victoria, Hensmann Meike, Molloy Sile, Sepulveda Nuno, Clark Taane G, Band Gavin, Clarke Geraldine M, Spencer Christopher C A, Kerasidou Angeliki, Campino Susana, Auburn Sarah, Tall Adama, Ly Alioune Badara, Mercereau-Puijalon Odile, Sakuntabhai Anavaj, Djimdé Abdoulaye, Maiga Boubacar, Touré Ousmane, Doumbo Ogobara K, Dolo Amagana, Troye-Blomberg Marita, Mangano Valentina D, Verra Frederica, Modiano David, Bougouma Edith, Sirima Sodiomon B, Ibrahim Muntaser, Hussain Ayman, Eid Nahid, Elzein Abier, Mohammed Hiba, Elhassan Ahmed, Elhassan Ibrahim, Williams Thomas N, Ndila Carolyne, Macharia Alexander, Marsh Kevin, Manjurano Alphaxard, Reyburn Hugh, Lemnge Martha, Ishengoma Deus, Carter Richard, Karunaweera Nadira, Fernando Deepika, Dewasurendra Rajika, Drakeley Christopher J, Riley Eleanor M, Kwiatkowski Dominic P, Rockett Kirk A
Wellcome Trust Centre for Human Genetics, University of Oxford, Roosevelt Drive, Oxford, UK.
London School of Hygiene and Tropical Medicine, Keppel Street, London, UK.
Malar J. 2015 Aug 28;14:333. doi: 10.1186/s12936-015-0833-x.
Many studies report associations between human genetic factors and immunity to malaria but few have been reliably replicated. These studies are usually country-specific, use small sample sizes and are not directly comparable due to differences in methodologies. This study brings together samples and data collected from multiple sites across Africa and Asia to use standardized methods to look for consistent genetic effects on anti-malarial antibody levels.
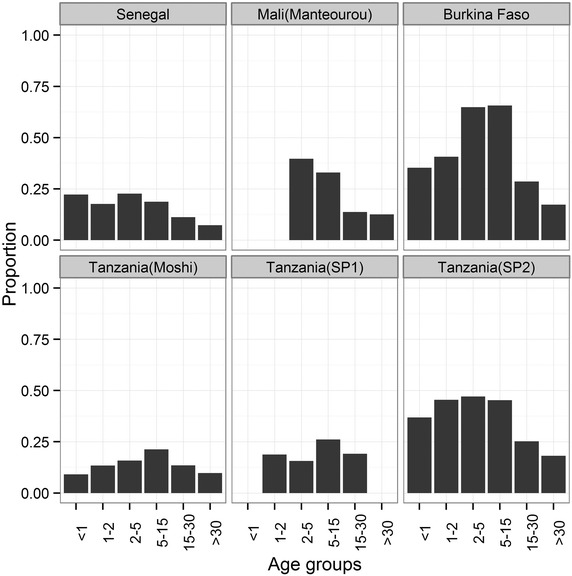
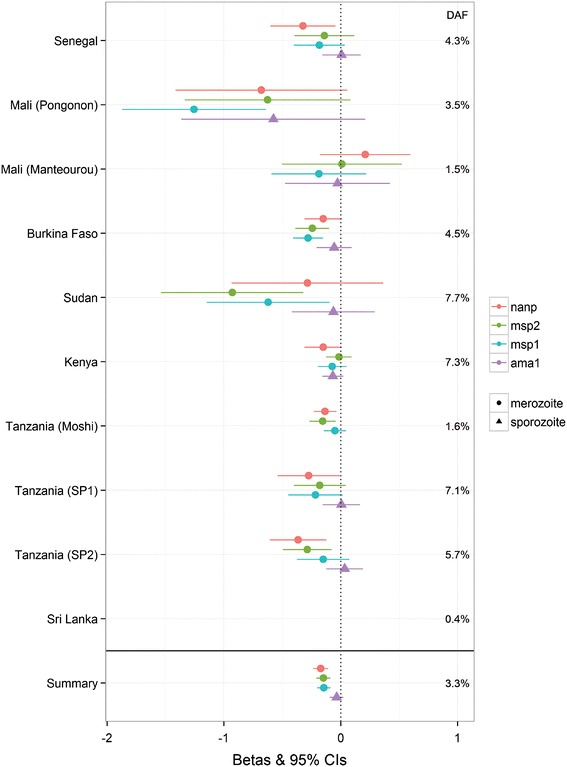
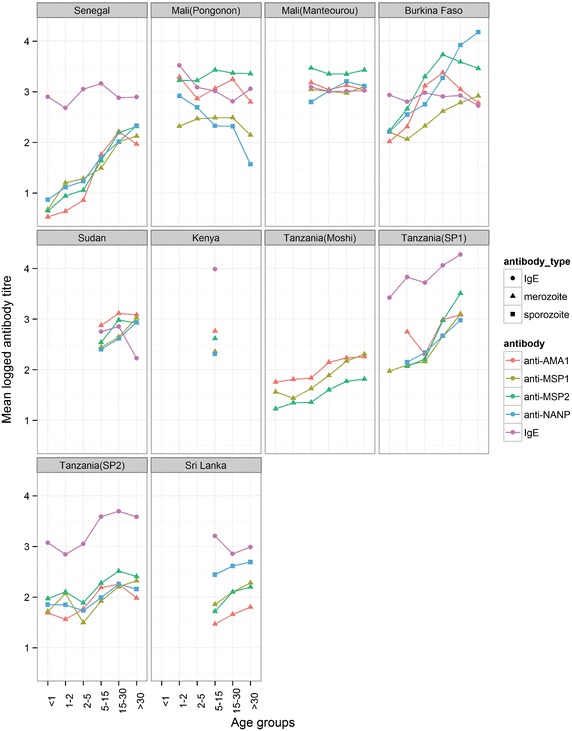
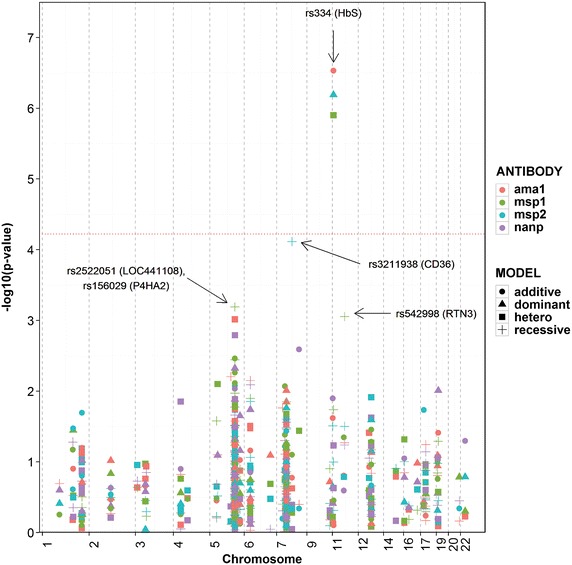
Sera, DNA samples and clinical data were collected from 13,299 individuals from ten sites in Senegal, Mali, Burkina Faso, Sudan, Kenya, Tanzania, and Sri Lanka using standardized methods. DNA was extracted and typed for 202 Single Nucleotide Polymorphisms with known associations to malaria or antibody production, and antibody levels to four clinical grade malarial antigens [AMA1, MSP1, MSP2, and (NANP)4] plus total IgE were measured by ELISA techniques. Regression models were used to investigate the associations of clinical and genetic factors with antibody levels.
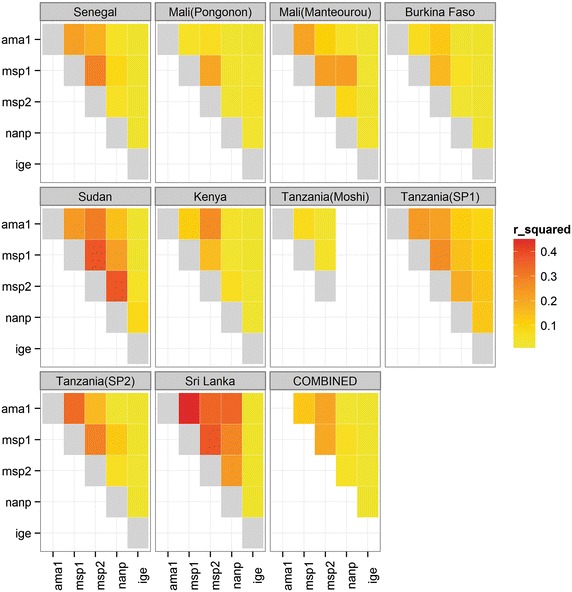
Malaria infection increased levels of antibodies to malaria antigens and, as expected, stable predictors of anti-malarial antibody levels included age, seasonality, location, and ethnicity. Correlations between antibodies to blood-stage antigens AMA1, MSP1 and MSP2 were higher between themselves than with antibodies to the (NANP)4 epitope of the pre-erythrocytic circumsporozoite protein, while there was little or no correlation with total IgE levels. Individuals with sickle cell trait had significantly lower antibody levels to all blood-stage antigens, and recessive homozygotes for CD36 (rs321198) had significantly lower anti-malarial antibody levels to MSP2.
Although the most significant finding with a consistent effect across sites was for sickle cell trait, its effect is likely to be via reducing a microscopically positive parasitaemia rather than directly on antibody levels. However, this study does demonstrate a framework for the feasibility of combining data from sites with heterogeneous malaria transmission levels across Africa and Asia with which to explore genetic effects on anti-malarial immunity.
许多研究报告了人类遗传因素与疟疾免疫力之间的关联,但很少有研究得到可靠的重复验证。这些研究通常是针对特定国家的,样本量较小,并且由于方法上的差异而无法直接进行比较。本研究汇集了从非洲和亚洲多个地点收集的样本和数据,采用标准化方法来寻找对抗疟抗体水平一致的遗传效应。
使用标准化方法从塞内加尔、马里、布基纳法索、苏丹、肯尼亚、坦桑尼亚和斯里兰卡的10个地点的13299名个体中收集血清、DNA样本和临床数据。提取DNA并对202个已知与疟疾或抗体产生相关的单核苷酸多态性进行分型,通过酶联免疫吸附测定技术测量针对四种临床级疟疾抗原[AMA1、MSP1、MSP2和(NANP)4]以及总IgE的抗体水平。使用回归模型研究临床和遗传因素与抗体水平之间的关联。
疟疾感染增加了针对疟疾抗原的抗体水平,正如预期的那样,抗疟抗体水平的稳定预测因素包括年龄、季节性、地理位置和种族。针对血液阶段抗原AMA1、MSP1和MSP2的抗体之间的相关性高于它们与针对红细胞前期环子孢子蛋白(NANP)4表位的抗体之间的相关性,而与总IgE水平几乎没有或没有相关性。具有镰状细胞性状的个体针对所有血液阶段抗原的抗体水平显著较低,而CD36(rs321198)的隐性纯合子针对MSP2的抗疟抗体水平显著较低。
尽管在各地点具有一致效应的最显著发现是镰状细胞性状,但其效应可能是通过减少显微镜下阳性的寄生虫血症,而不是直接作用于抗体水平。然而,本研究确实展示了一个框架,用于将来自非洲和亚洲疟疾传播水平各异的地点的数据结合起来,以探索遗传因素对抗疟免疫力的影响,该框架具有可行性。