Samson Pamela, Patel Aalok, Robinson Cliff G, Morgensztern Daniel, Chang Su-Hsin, Colditz Graham A, Waqar Saiama, Crabtree Traves D, Krupnick A Sasha, Kreisel Daniel, Patterson G Alexander, Meyers Bryan F, Puri Varun
Division of Cardiothoracic Surgery, Washington University in St. Louis School of Medicine, St. Louis, Missouri.
Department of Radiation Oncology, Washington University in St. Louis School of Medicine, St. Louis, Missouri.
Ann Thorac Surg. 2015 Dec;100(6):2026-32; discussion 2032. doi: 10.1016/j.athoracsur.2015.05.091. Epub 2015 Aug 25.
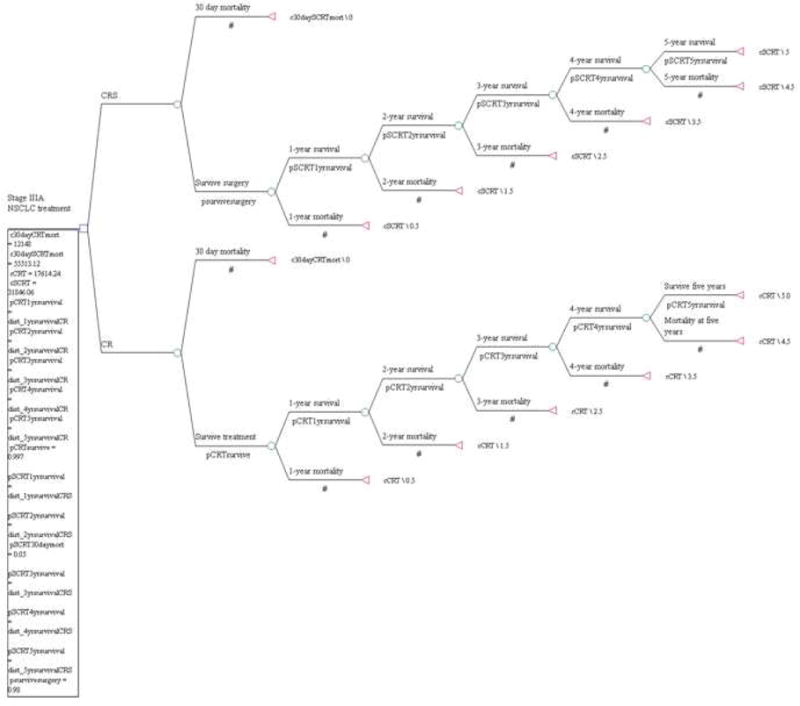
This study evaluated the cost-effectiveness of combination chemotherapy, radiotherapy, and surgical intervention (CRS) vs definitive chemotherapy and radiotherapy (CR) in clinical stage IIIA non-small cell lung cancer (NSCLC) patients at academic and nonacademic centers.
Patients with clinical stage IIIA NSCLC receiving CR or CRS from 1998 to 2010 were identified in the National Cancer Data Base. Propensity score matching on patient, tumor, and treatment characteristics was performed. Medicare allowable charges were used for treatment costs. The incremental cost-effectiveness ratio (ICER) was based on probabilistic 5-year survival and calculated as cost per life-year gained.
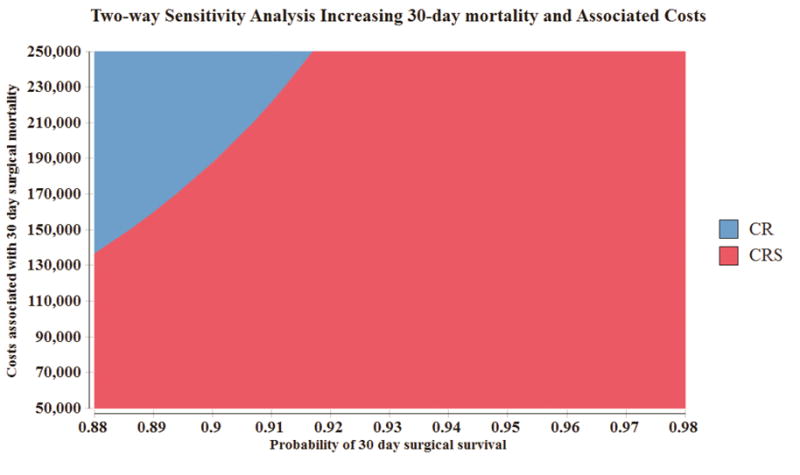
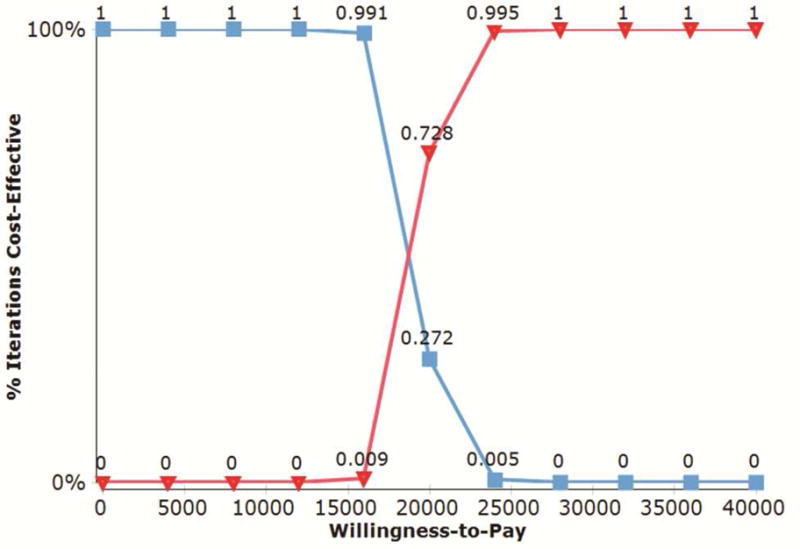
We identified 5,265 CR and CRS matched patient pairs. Surgical resection imparted an increased effectiveness of 0.83 life-years, with an ICER of $17,618. Among nonacademic centers, 1,634 matched CR and CRS patients demonstrated a benefit with surgical resection of 0.86 life-years gained, for an ICER of $17,124. At academic centers, 3,201 matched CR and CRS patients had increased survival of 0.81 life-years with surgical resection, for an ICER of $18,144. Finally, 3,713 CRS patients were matched between academic and nonacademic centers. Academic center surgical patients had an increased effectiveness of 1.5 months gained and dominated the model with lower surgical cost estimates associated with lower 30-day mortality rates.
In stage IIIA NSCLC, the selective addition of surgical resection to CR is cost-effective compared with definitive chemoradiation therapy at nonacademic and academic centers. These conclusions are valid over a range of clinically meaningful variations in cost and treatment outcomes.
本研究评估了在学术中心和非学术中心,联合化疗、放疗及手术干预(CRS)与单纯根治性化疗和放疗(CR)相比,对临床ⅢA期非小细胞肺癌(NSCLC)患者的成本效益。
在国家癌症数据库中识别出1998年至2010年接受CR或CRS治疗的临床ⅢA期NSCLC患者。根据患者、肿瘤和治疗特征进行倾向评分匹配。使用医疗保险允许的费用作为治疗成本。增量成本效益比(ICER)基于概率性5年生存率计算,以每获得一个生命年的成本来表示。
我们识别出5265对匹配的CR和CRS患者。手术切除使有效生存期增加了0.83个生命年,ICER为17618美元。在非学术中心,1634对匹配的CR和CRS患者显示手术切除带来了0.86个生命年的获益,ICER为17124美元。在学术中心,3201对匹配的CR和CRS患者手术切除后生存期增加了0.81个生命年,ICER为18144美元。最后,在学术中心和非学术中心之间匹配了3713例接受CRS治疗的患者。学术中心的手术患者有效生存期增加了1.5个月,且以较低的手术成本估计和较低的30天死亡率在模型中占优。
在ⅢA期NSCLC中,与非学术中心和学术中心的单纯根治性放化疗相比,在CR基础上选择性增加手术切除具有成本效益。这些结论在成本和治疗结果的一系列具有临床意义的变化范围内都是有效的。