Avallone Antonio, Pecori Biagio, Bianco Franco, Aloj Luigi, Tatangelo Fabiana, Romano Carmela, Granata Vincenza, Marone Pietro, Leone Alessandra, Botti Gerardo, Petrillo Antonella, Caracò Corradina, Iaffaioli Vincenzo R, Muto Paolo, Romano Giovanni, Comella Pasquale, Budillon Alfredo, Delrio Paolo
Gastrointestinal Medical Oncology Unit, Istituto Nazionale per lo Studio e la Cura dei Tumori "Fondazione Giovanni Pascale" - IRCCS, 80131, Napoli, Italy.
Radiotherapy Unit, Istituto Nazionale per lo Studio e la Cura dei Tumori "Fondazione Giovanni Pascale" - IRCCS, 80131, Napoli, Italy.
Oncotarget. 2015 Oct 6;6(30):30394-407. doi: 10.18632/oncotarget.4724.
We have previously shown that an intensified preoperative regimen including oxaliplatin plus raltitrexed and 5-fluorouracil/folinic acid (OXATOM/FUFA) during preoperative pelvic radiotherapy produced promising results in locally advanced rectal cancer (LARC). Preclinical evidence suggests that the scheduling of bevacizumab may be crucial to optimize its combination with chemo-radiotherapy.
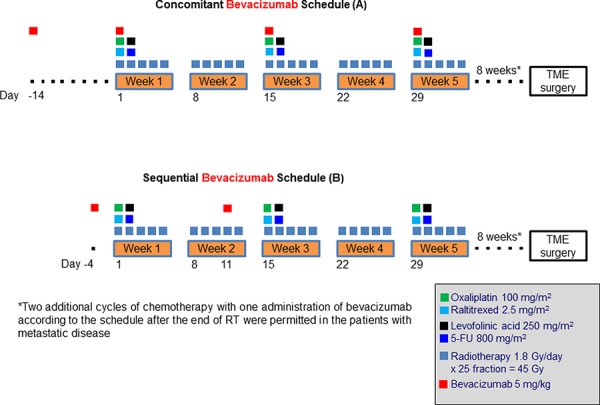
This non-randomized, non-comparative, phase II study was conducted in MRI-defined high-risk LARC. Patients received three biweekly cycles of OXATOM/FUFA during RT. Bevacizumab was given 2 weeks before the start of chemo-radiotherapy, and on the same day of chemotherapy for 3 cycles (concomitant-schedule A) or 4 days prior to the first and second cycle of chemotherapy (sequential-schedule B). Primary end point was pathological complete tumor regression (TRG1) rate.
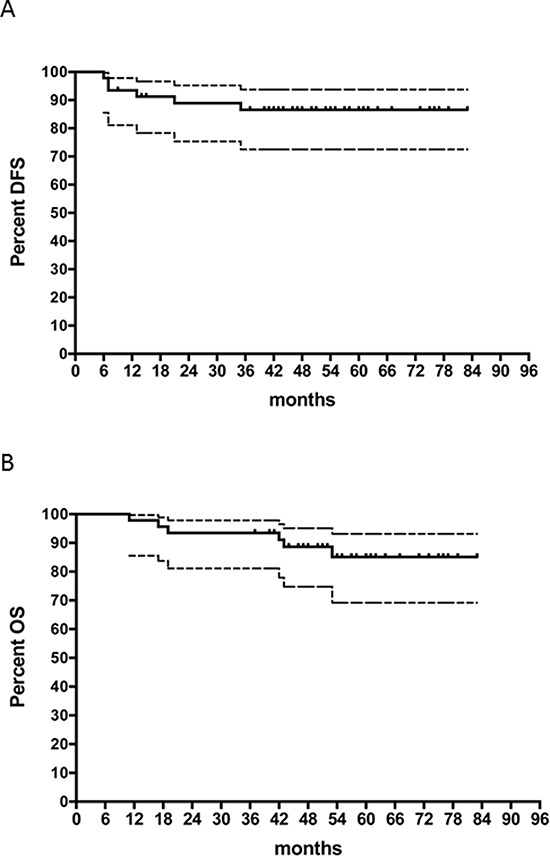
The accrual for the concomitant-schedule was early terminated because the number of TRG1 (2 out of 16 patients) was statistically inconsistent with the hypothesis of activity (30%) to be tested. Conversely, the endpoint was reached with the sequential-schedule and the final TRG1 rate among 46 enrolled patients was 50% (95% CI 35%-65%). Neutropenia was the most common grade ≥ 3 toxicity with both schedules, but it was less pronounced with the sequential than concomitant-schedule (30% vs. 44%). Postoperative complications occurred in 8/15 (53%) and 13/46 (28%) patients in schedule A and B, respectively. At 5 year follow-up the probability of PFS and OS was 80% (95%CI, 66%-89%) and 85% (95%CI, 69%-93%), respectively, for the sequential-schedule.
These results highlights the relevance of bevacizumab scheduling to optimize its combination with preoperative chemo-radiotherapy in the management of LARC.
我们之前已经表明,在术前盆腔放疗期间采用强化术前方案,包括奥沙利铂联合雷替曲塞以及5-氟尿嘧啶/亚叶酸(OXATOM/FUFA),在局部晚期直肠癌(LARC)治疗中取得了有前景的结果。临床前证据表明,贝伐单抗的给药时机对于优化其与放化疗联合可能至关重要。
这项非随机、非对照的II期研究在MRI定义的高危LARC患者中进行。患者在放疗期间接受三个每两周一次的OXATOM/FUFA周期治疗。贝伐单抗在放化疗开始前2周给药,并在化疗的同一天给药3个周期(同步给药方案A),或在化疗的第一和第二周期前4天给药(序贯给药方案B)。主要终点是病理完全肿瘤消退(TRG1)率。
同步给药方案的入组提前终止,因为TRG1患者数量(16例患者中有2例)在统计学上与要测试的活性假设(30%)不一致。相反,序贯给药方案达到了终点,46例入组患者的最终TRG1率为50%(95%CI 35%-65%)。中性粒细胞减少是两种给药方案中最常见的≥3级毒性反应,但序贯给药方案比同步给药方案的症状轻(30%对44%)。A组和B组分别有8/15(53%)和13/46(28%)的患者发生术后并发症。在5年随访中,序贯给药方案的无进展生存期(PFS)和总生存期(OS)概率分别为80%(95%CI,66%-89%)和85%(95%CI,69%-93%)。
这些结果凸显了贝伐单抗给药时机对于优化其与术前放化疗联合治疗LARC的相关性。