Service de Chirurgie Digestive et Oncologique, Hôpital Bicêtre, Groupe Hospitalier Universitaire Paris Sud, Assistance Publique, Hôpitaux de Paris, 63, rue Gabriel Péri, Le Kremlin Bicetre, 94275, France.
Faculté de Médecine Paris Sud, Université Paris Saclay, Lrekmlin Bicêtre, 94275, France.
BMC Cancer. 2020 May 29;20(1):485. doi: 10.1186/s12885-020-06968-1.
Preoperative radiochemotherapy (RCT) is recommended in France prior to total mesorectal excision in patients with mid or low locally advanced rectal cancer (LARC) (cT3/T4 and/or N+) because it has been shown to improve local control. Preoperative RCT has also disadvantages including the absence of proven impact on metastatic recurrence and the risk of late side effects on bowel and genitourinary function. In patients with primarily resectable LARC, preoperative systemic chemotherapy without pelvic irradiation could be used as an alternative to RCT.
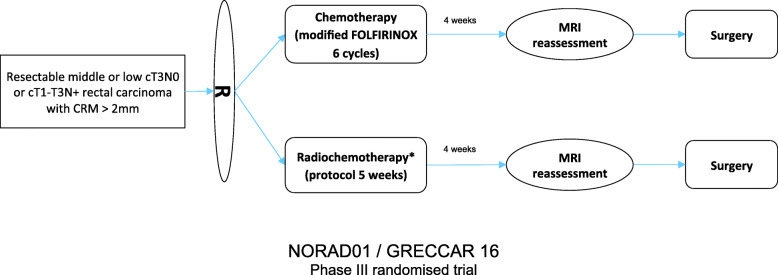
This study is a multicenter, open-label randomized, 2-arm phase III non-inferiority trial. Patients with mid or low resectable LARC (cT3N0 or cT1-T3N+ with circumferential resection margin [CRM] > 2 mm on pretreatment MRI) will be randomized to either modified FOLFIRINOX for 3 months or RCT (Cap50 intensified-modulated radiotherapy). All patients have restaging MRI after preoperative treatment. The primary endpoint is 3-year progression-free survival (PFS) from the time to randomization including progression during preoperative treatment. Secondary endpoints are treatment related toxicity, treatment compliance, R0 resection rate, sphincter saving surgery rate, postoperative morbidity and mortality rates, loco-regional recurrence free survival, overall survival, bowel and sexual functions at diagnosis, quality of life, radiologic and pathologic response after preoperative treatment. The number of patients required is 574.
The choice of modified FOLFIRINOX for preoperative chemotherapy is supported by recent and consistent data on safety and efficacy of this regimen on rectal cancer. The use of preoperative chemotherapy instead of RCT could be associated with pronounced advantages in terms of functional results and quality of life in cancer survivors. However and first of all, the non-inferiority of preoperative chemotherapy compared to RCT on oncologic outcome has to be validated. If this study demonstrates the non-inferiority of chemotherapy compared to RCT, this can lead to a crucial change in clinical practice in a large subset of rectal cancer patients.
ClinicalTrials.gov NCT03875781 (March 15, 2019). Version 1.1.
术前放化疗(RCT)在法国被推荐用于中低位局部晚期直肠癌(LARC)(cT3/T4 和/或 N+)患者的全直肠系膜切除术前,因为它已被证明可提高局部控制率。术前 RCT 也有缺点,包括对转移性复发没有明显影响,以及对肠道和泌尿生殖功能的迟发性副作用的风险。对于主要可切除的 LARC 患者,可替代 RCT 使用术前全身化疗而不进行盆腔照射。
这是一项多中心、开放性、随机、2 臂、III 期非劣效性试验。中低位可切除的 LARC(cT3N0 或 cT1-T3N+,术前 MRI 显示环周切缘 [CRM]>2mm)患者将被随机分配至接受改良 FOLFIRINOX 治疗 3 个月或 RCT(Cap50 强化调强放疗)。所有患者在术前治疗后进行重新分期 MRI。主要终点是从随机分组时间起的 3 年无进展生存(PFS),包括术前治疗期间的进展。次要终点是治疗相关毒性、治疗依从性、R0 切除率、保肛手术率、术后发病率和死亡率、局部无复发生存率、总生存率、诊断时的肠道和性功能、生活质量、术前治疗后的影像学和病理学反应。需要的患者人数为 574 人。
改良 FOLFIRINOX 用于术前化疗的选择得到了最近关于该方案在直肠癌安全性和有效性的一致数据的支持。与 RCT 相比,使用术前化疗可能在癌症幸存者的功能结果和生活质量方面具有明显优势。然而,首先,术前化疗在肿瘤学结果方面与 RCT 的非劣效性必须得到验证。如果这项研究证明化疗与 RCT 相比不劣效,这可能会导致直肠癌患者的临床实践发生重大变化。
ClinicalTrials.gov NCT03875781(2019 年 3 月 15 日)。版本 1.1。