Chang Kun, Qin Xiao-Jian, Zhang Hai-Liang, Dai Bo, Zhu Yao, Shi Guo-Hai, Shen Yi-Jun, Zhu Yi-Ying, Ye Ding-Wei
Department of Urology, Fudan University Shanghai Cancer Center, Shanghai 200032, China.
Asian J Androl. 2016 May-Jun;18(3):452-5. doi: 10.4103/1008-682X.160884.
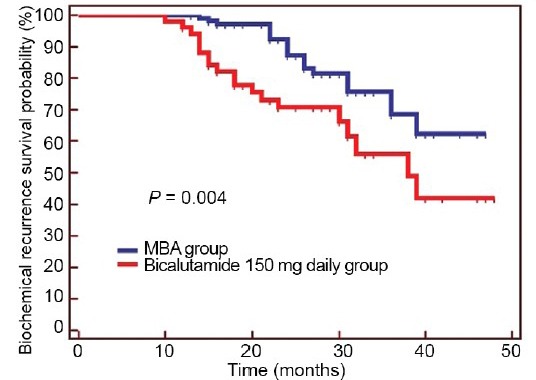
The role of adjuvant hormonal therapy and optimized regimens for high-risk localized prostate cancer after radical prostatectomy remains controversial. Herein, the clinical trial CU1005 prospectively evaluated two regimens of maximum androgen blockage or bicalutamide 150 mg daily as immediate adjuvant therapy for high-risk localized prostate cancer. Overall, 209 consecutive patients were recruited in this study, 107 of whom received 9 months of adjuvant maximum androgen blockage, whereas 102 received 9 months of adjuvant bicalutamide 150 mg. The median postoperative follow-up time was 27.0 months. The primary endpoint was biochemical recurrence. Of the 209 patients, 59 patients developed biochemical recurrence. There was no difference between the two groups with respect to clinical characteristics, including age, pretreatment prostate-specific antigen, Gleason score, surgical margin status, or pathological stages. The maximum androgen blockage group experienced longer biochemical recurrence-free survival (P = 0.004) compared with the bicalutamide 150 mg group. Side-effects in the two groups were similar and could be moderately tolerated in all patients. In conclusion, immediate, 9-month maximum androgen blockage should be considered as an alternative to bicalutamide 150 mg as adjuvant treatment for high-risk localized prostate cancer patients after radical prostatectomy.
辅助激素治疗以及根治性前列腺切除术后高危局限性前列腺癌的优化方案的作用仍存在争议。在此,临床试验CU1005前瞻性地评估了两种方案,即最大雄激素阻断或每日150 mg比卡鲁胺作为高危局限性前列腺癌的即刻辅助治疗。总体而言,本研究连续招募了209例患者,其中107例接受了9个月的辅助最大雄激素阻断治疗,而102例接受了9个月的辅助每日150 mg比卡鲁胺治疗。术后中位随访时间为27.0个月。主要终点是生化复发。在这209例患者中,有59例发生了生化复发。两组在临床特征方面无差异,包括年龄、治疗前前列腺特异性抗原、Gleason评分、手术切缘状态或病理分期。与每日150 mg比卡鲁胺组相比,最大雄激素阻断组的生化无复发生存期更长(P = 0.004)。两组的副作用相似,所有患者均可适度耐受。总之,对于根治性前列腺切除术后的高危局限性前列腺癌患者,应考虑将即刻9个月的最大雄激素阻断作为每日150 mg比卡鲁胺辅助治疗的替代方案。