Raghavan S, Geller S, Miller S, Goudar S S, Anger H, Yadavannavar M C, Dabash R, Bidri S R, Gudadinni M R, Udgiri R, Koch A R, Bellad M B, Winikoff B
Gynuity Health Projects, New York, NY, USA.
University of Illinois at Chicago, Chicago, IL, USA.
BJOG. 2016 Jan;123(1):120-7. doi: 10.1111/1471-0528.13540. Epub 2015 Sep 1.
To assess whether secondary prevention, which preemptively treats women with above-average postpartum bleeding, is non-inferior to universal prophylaxis.
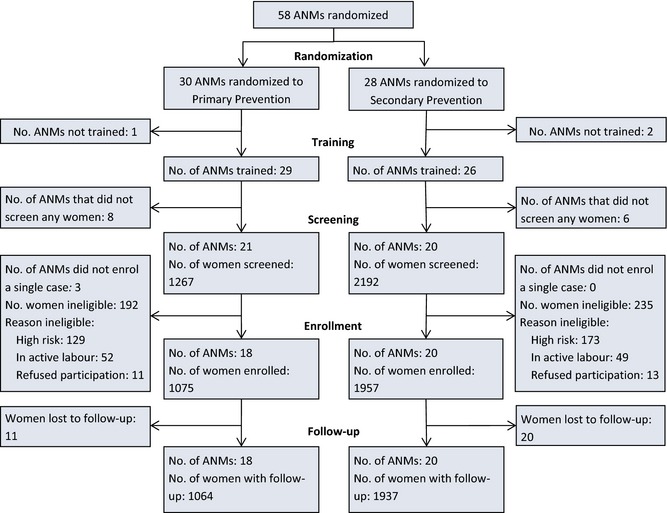
A cluster-randomised non-inferiority community trial.
Health sub-centres and home deliveries in the Bijapur district of Karnataka, India.
Women with low-risk pregnancies who were eligible for delivery with an Auxiliary Nurse Midwife at home or sub-centre and who consented to be part of the study.
Auxiliary Nurse Midwifes were randomised to secondary prevention using 800 mcg sublingual misoprostol administered to women with postpartum blood loss ≥350 ml or to universal prophylaxis using 600 mcg oral misoprostol administered to all women during the third stage of labour.
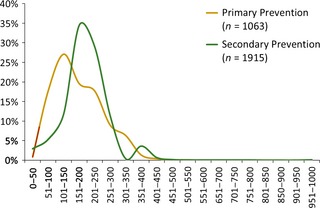
Postpartum haemoglobin ≤7.8 g/dl, mean postpartum blood loss and postpartum haemoglobin, postpartum haemorrhage rate, transfer to higher-level facilities, acceptability and feasibility of the intervention.
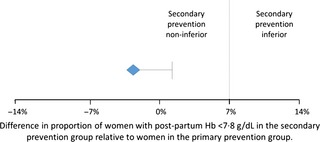
Misoprostol was administered to 99.7% of women as primary prevention. In secondary prevention, 92 (4.7%) women had postpartum bleeding ≥350 ml, of which 90 (97.8%) received misoprostol. The proportion of women with postpartum haemoglobin ≤7.8 g/dl was 5.9 and 8.8% in secondary and primary prevention clusters, respectively [difference -2.9%, one-sided 95% confidence interval (CI) <1.3%]. Postpartum transfer and haemorrhage rates were low (<1%) in both groups. Shivering was more common in primary prevention clusters (P = 0.013).
Secondary prevention of postpartum haemorrhage with misoprostol is non-inferior to universal prophylaxis based on the primary outcome of postpartum haemoglobin. Secondary prevention could be a good alternative to universal prophylaxis as it medicates fewer women and is an acceptable and feasible strategy at the community level.
Secondary prevention of postpartum haemorrhage with misoprostol is non-inferior to universal prophylaxis.
评估对产后出血高于平均水平的女性进行预先治疗的二级预防是否不劣于普遍预防。
一项整群随机非劣效性社区试验。
印度卡纳塔克邦比贾布尔区的卫生分中心和家庭分娩。
低风险妊娠且有资格由辅助护士助产士在家中或卫生分中心分娩并同意参与研究的女性。
辅助护士助产士被随机分配进行二级预防(对产后失血≥350毫升的女性舌下含服800微克米索前列醇)或普遍预防(在第三产程对所有女性口服600微克米索前列醇)。
产后血红蛋白≤7.8克/分升、平均产后失血量和产后血红蛋白、产后出血率、转至上级医疗机构情况、干预措施的可接受性和可行性。
99.7%的女性接受了米索前列醇作为一级预防。在二级预防中,92名(4.7%)女性产后出血≥350毫升,其中90名(97.8%)接受了米索前列醇。二级预防组和一级预防组中产后血红蛋白≤7.8克/分升的女性比例分别为5.9%和8.8%[差异-2.9%,单侧95%置信区间(CI)<1.3%]。两组的产后转诊和出血率均较低(<1%)。寒战在一级预防组中更常见(P=0.013)。
基于产后血红蛋白这一主要结局,米索前列醇对产后出血的二级预防不劣于普遍预防。二级预防可能是普遍预防的一个良好替代方案,因为用药的女性较少,且在社区层面是一种可接受且可行的策略。
米索前列醇对产后出血的二级预防不劣于普遍预防。