Artlett Carol M, Sassi-Gaha Sihem, Ramos Ronald C, Miller Frederick W, Rider Lisa G
Department of Microbiology and Immunology, Drexel University College of Medicine, 2900 Queen Lane, Philadelphia, PA, 19129, USA.
Department of Medicine, Thomas Jefferson University, 1020 Walnut Street, Philadelphia, PA, 19107, USA.
Arthritis Res Ther. 2015 Sep 4;17(1):238. doi: 10.1186/s13075-015-0732-0.
Microchimeric cells have been studied for over a decade, with conflicting reports on their presence and role in autoimmune and other inflammatory diseases. To determine whether microchimeric cells were pathogenic or mediating tissue repair in inflammatory myopathies, we phenotyped and quantified microchimeric cells in juvenile idiopathic inflammatory myopathies (JIIM), muscular dystrophy (MD), and noninflammatory control muscle tissues.
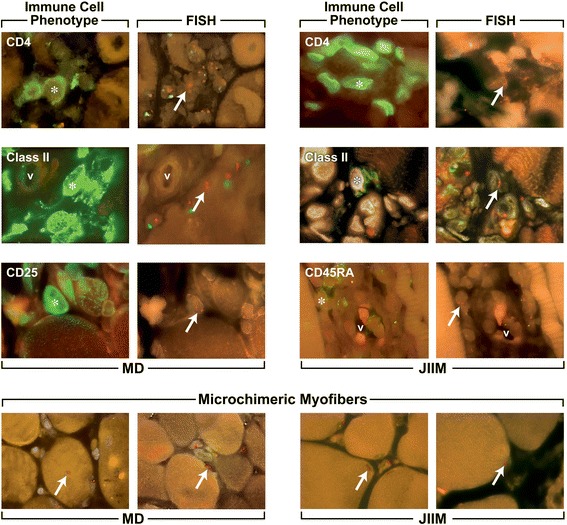
Fluorescence immunophenotyping for infiltrating cells with sequential fluorescence in situ hybridization was performed on muscle biopsies from ten patients with JIIM, nine with MD and ten controls.
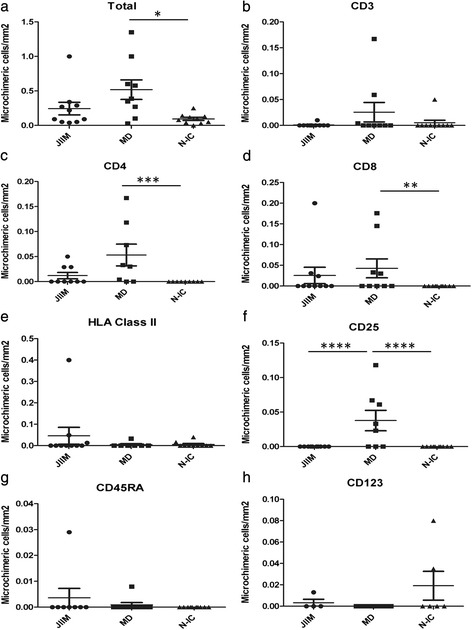
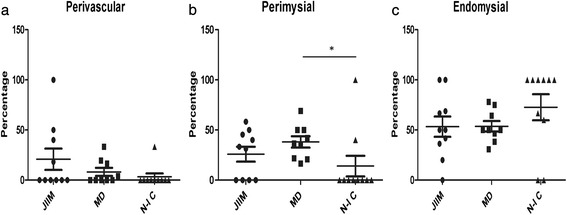
Microchimeric cells were significantly increased in MD muscle (0.079 ± 0.024 microchimeric cells/mm(2) tissue) compared to controls (0.019 ± 0.007 cells/mm(2) tissue, p = 0.01), but not elevated in JIIM muscle (0.043 ± 0.015 cells/mm(2)). Significantly more CD4+ and CD8+ microchimeric cells were in the muscle of patients with MD compared with controls (mean 0.053 ± 0.020/mm(2) versus 0 ± 0/mm(2) p = 0.003 and 0.043 ± 0.023/mm(2) versus 0 ± 0/mm(2) p = 0.025, respectively). No differences in microchimeric cells between JIIM, MD, and noninflammatory controls were found for CD3+, Class II+, CD25+, CD45RA+, and CD123+ phenotypes, and no microchimeric cells were detected in CD20, CD83, or CD45RO populations. The locations of microchimeric cells were similar in all three conditions, with MD muscle having more microchimeric cells in perimysial regions than controls, and JIIM having fewer microchimeric muscle nuclei than MD. Microchimeric inflammatory cells were found, in most cases, at significantly lower proportions than autologous cells of the same phenotype.
Microchimeric cells are not specific to autoimmune disease, and may not be important in muscle inflammation or tissue repair in JIIM.
微嵌合细胞已被研究了十多年,关于它们在自身免疫性疾病和其他炎症性疾病中的存在及作用,报告结果相互矛盾。为了确定微嵌合细胞在炎性肌病中是致病的还是介导组织修复的,我们对青少年特发性炎性肌病(JIIM)、肌肉营养不良(MD)和非炎性对照肌肉组织中的微嵌合细胞进行了表型分析和定量。
对10例JIIM患者、9例MD患者和10例对照的肌肉活检组织进行连续荧光原位杂交,对浸润细胞进行荧光免疫表型分析。
与对照组(0.019±0.007个微嵌合细胞/mm²组织,p = 0.01)相比,MD肌肉中的微嵌合细胞显著增加(0.079±0.024个微嵌合细胞/mm²组织),但JIIM肌肉中的微嵌合细胞未升高(0.043±0.015个细胞/mm²)。与对照组相比,MD患者肌肉中的CD4⁺和CD8⁺微嵌合细胞明显更多(分别为平均0.053±0.020/mm²对0±0/mm²,p = 0.003;0.043±0.023/mm²对0±0/mm²,p = 0.025)。在JIIM、MD和非炎性对照之间,CD3⁺、II类⁺、CD25⁺、CD45RA⁺和CD123⁺表型的微嵌合细胞没有差异,在CD20、CD83或CD45RO群体中未检测到微嵌合细胞。在所有三种情况下,微嵌合细胞的位置相似,MD肌肉中肌束膜区域的微嵌合细胞比对照组更多,而JIIM中微嵌合肌核比MD更少。在大多数情况下,发现微嵌合炎性细胞的比例明显低于相同表型的自体细胞。
微嵌合细胞并非自身免疫性疾病所特有,并可能在JIIM的肌肉炎症或组织修复中并不重要。