Kang Moon Hyung, Yu Young Dong, Shin Hyun Soo, Oh Jong Jin, Park Dong Soo
Department of Urology, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
Department of Radiation Oncology, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
Korean J Urol. 2015 Sep;56(9):637-43. doi: 10.4111/kju.2015.56.9.637. Epub 2015 Sep 2.
To investigate the difference in rectal complications rate following prostate low dose rate (LDR) brachytherapy based on prostate-rectum distance and prostate longitudinal length among early prostate cancer patients.
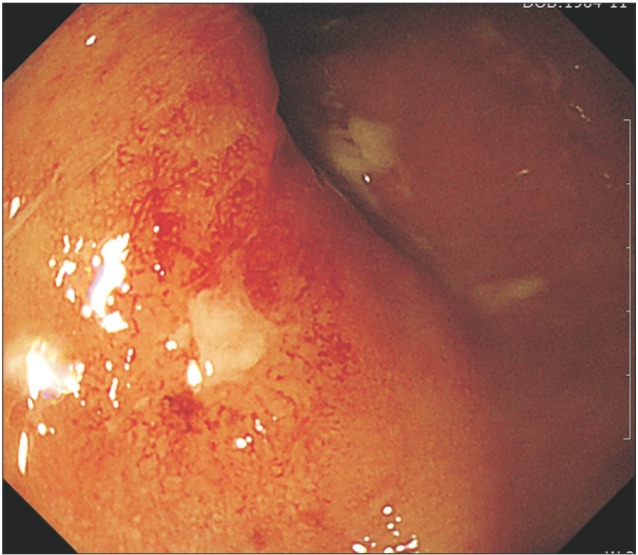
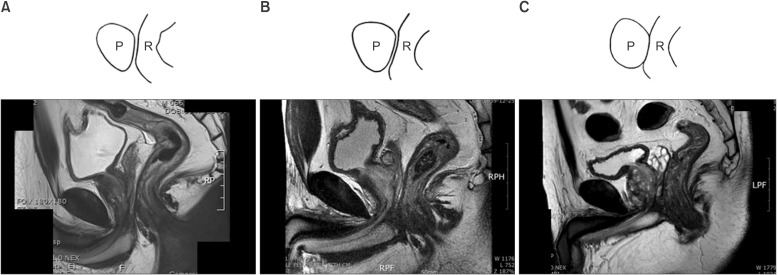
From March 2008 to February 2013, 245 prostate cancer patients with a Gleason score ≤7 were treated with 125-I LDR brachytherapy. Among them, 178 patients with prostate volume 20-35 mL and a follow-up period ≥6 months were evaluated for radiation proctitis. Magnetic resonance imaging (MRI) was performed for a prebrachytherapy evaluation, and prostate-rectum distance and prostate longitudinal length were measured. The radiation proctitis was confirmed and graded via colonoscopy based on the radiation therapy oncology group (RTOG) toxicity criteria.
Twenty-three patients received a colonoscopy for proctitis evaluation, and 12 were identified as grade 1 on the RTOG scale. Nine patients were diagnosed as grade 2 and 2 patients were grade 3. No patient developed grade 4 proctitis. The rectal-complication group had a mean prostate-rectum distance of 2.51±0.16 mm, while non-rectal-complication control group had 3.32±0.31 mm. The grade 1 proctitis patients had a mean prostate-rectum distance of 2.80±0.15 mm, which was significantly longer than 2.12±0.31 mm of grades 2 and 3 patient groups (p=0.045). All 11 patients of grades 2 and 3 had a prostate longitudinal length of 35.22±2.50 mm, which was longer than group 1, but the difference was not statistically significant (p=0.214).
As the prostate-rectum distance increased, fewer postimplantation rectal symptoms were observed. Patients with a shorter prostate-rectum distance in MRI should receive modified implantation techniques or radical prostatectomy.
探讨早期前列腺癌患者中,基于前列腺与直肠的距离以及前列腺纵轴长度,前列腺低剂量率(LDR)近距离放射治疗后直肠并发症发生率的差异。
2008年3月至2013年2月,对245例Gleason评分≤7的前列腺癌患者进行¹²⁵I LDR近距离放射治疗。其中,对178例前列腺体积为20 - 35 mL且随访期≥6个月的患者进行放射性直肠炎评估。在近距离放射治疗前进行磁共振成像(MRI)评估,测量前列腺与直肠的距离以及前列腺纵轴长度。根据放射肿瘤学组(RTOG)毒性标准,通过结肠镜检查确认并分级放射性直肠炎。
23例患者接受结肠镜检查以评估直肠炎,其中12例在RTOG量表上被判定为1级。9例患者被诊断为2级,2例为3级。无患者发生4级直肠炎。直肠并发症组的前列腺与直肠平均距离为2.51±0.16 mm,而非直肠并发症对照组为3.32±0.31 mm。1级直肠炎患者的前列腺与直肠平均距离为2.80±0.15 mm,明显长于2级和3级患者组的2.12±0.31 mm(p = 0.045)。2级和3级的所有11例患者的前列腺纵轴长度为35.22±2.50 mm,长于1级组,但差异无统计学意义(p = 0.214)。
随着前列腺与直肠距离增加,植入后直肠症状较少。MRI检查中前列腺与直肠距离较短的患者应采用改良植入技术或根治性前列腺切除术。