Solomon Cristina, Ranucci Marco, Hochleitner Gerald, Schöchl Herbert, Schlimp Christoph J
From the CSL Behring, Marburg, Germany; Department of Anesthesiology, Perioperative Care and General Intensive Care, Paracelsus Medical University, Salzburg University Hospital, Salzburg, Austria; Ludwig Boltzmann Institute for Experimental and Clinical Traumatology and AUVA Research Centre, Vienna, Austria; Department of Cardiothoracic and Vascular Anesthesia and Intensive Care, IRCCS Policlinico, San Donato, Milan, Italy; CSL Behring, Vienna, Austria and Department of Anesthesiology and Intensive Care, AUVA Trauma Hospital of Salzburg, Austria.
Anesth Analg. 2015 Oct;121(4):868-878. doi: 10.1213/ANE.0000000000000859.
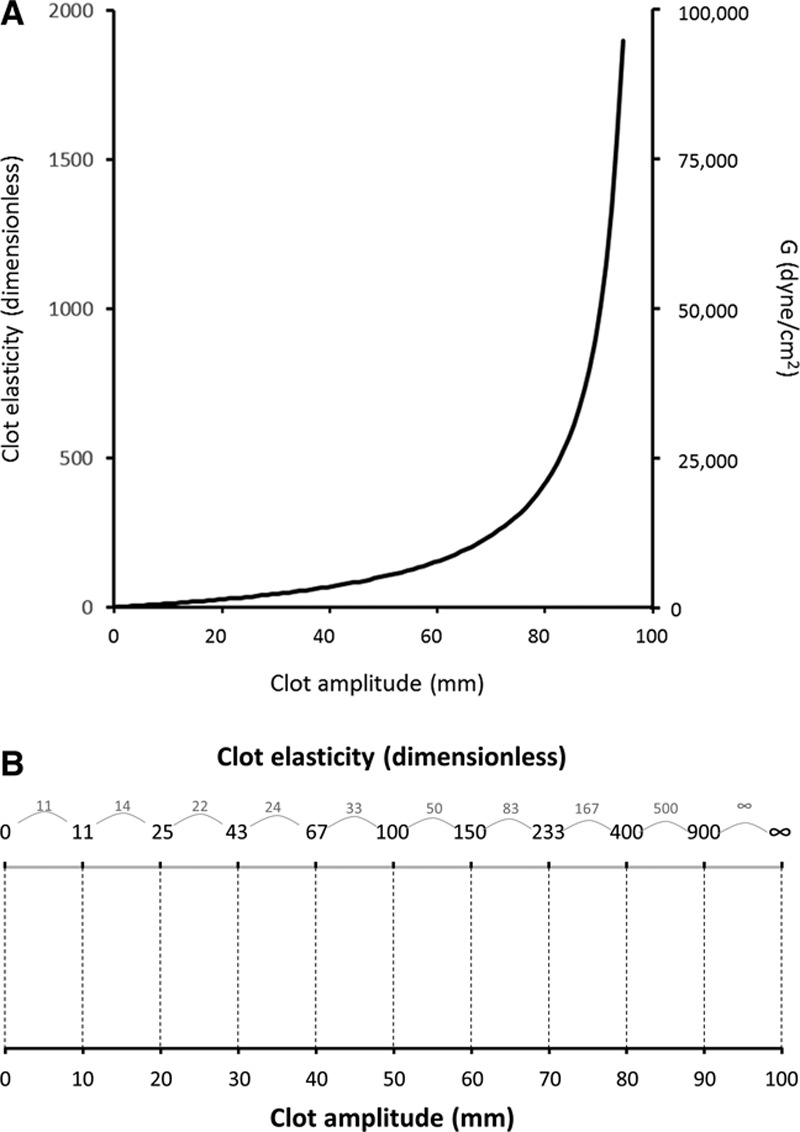
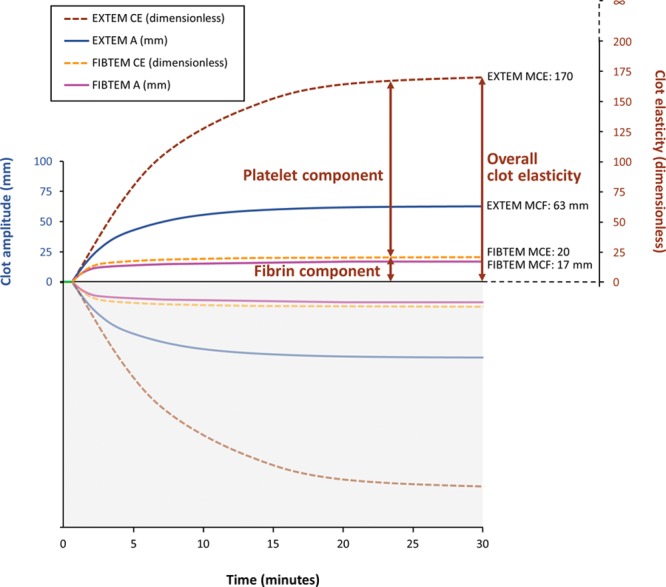
The viscoelastic properties of blood clot have been studied most commonly using thrombelastography (TEG) and thromboelastometry (ROTEM). ROTEM-based bleeding treatment algorithms recommend administering platelets to patients with low EXTEM clot strength (e.g., clot amplitude at 10 minutes [A10] <40 mm) once clot strength of the ROTEM® fibrin-based test (FIBTEM) is corrected. Algorithms based on TEG typically use a low value of maximum amplitude (e.g., <50 mm) as a trigger for administering platelets. However, this parameter reflects the contributions of various blood components to the clot, including platelets and fibrin/fibrinogen. The platelet component of clot strength may provide a more sensitive indication of platelet deficiency than clot amplitude from a whole blood TEG or ROTEM® assay. The platelet component of the formed clot is derived from the results of TEG/ROTEM® tests performed with and without platelet inhibition. In this article, we review the basis for why this calculation should be based on clot elasticity (e.g., the E parameter with TEG and the CE parameter with ROTEM®) as opposed to clot amplitude (e.g., the A parameter with TEG or ROTEM®). This is because clot elasticity, unlike clot amplitude, reflects the force with which the blood clot resists rotation within the device, and the relationship between clot amplitude (variable X) and clot elasticity (variable Y) is nonlinear. A specific increment of X (ΔX) will be associated with different increments of Y (ΔY), depending on the initial value of X. When calculated correctly, using clot elasticity data, the platelet component of the clot can provide a valuable insight into platelet deficiency in emergency bleeding.
对血凝块黏弹性特性的研究,最常用的方法是血栓弹力图(TEG)和血栓弹性测定法(ROTEM)。基于ROTEM的出血治疗算法建议,一旦ROTEM®纤维蛋白基检测(FIBTEM)的血凝强度得到校正,就应向EXTEM血凝强度低的患者(例如,10分钟时的血凝幅度[A10]<40mm)输注血小板。基于TEG的算法通常使用低的最大幅度值(例如,<50mm)作为输注血小板的触发指标。然而,该参数反映了包括血小板和纤维蛋白/纤维蛋白原在内的各种血液成分对血凝块的贡献。与全血TEG或ROTEM®检测的血凝幅度相比,血凝强度的血小板成分可能更能敏感地指示血小板缺乏情况。已形成血凝块的血小板成分来自于在有和没有血小板抑制的情况下进行的TEG/ROTEM®检测结果。在本文中,我们回顾了为什么这种计算应该基于血凝弹性(例如,TEG的E参数和ROTEM®的CE参数)而不是血凝幅度(例如,TEG或ROTEM®的A参数)的依据。这是因为与血凝幅度不同,血凝弹性反映了血凝块在仪器内抵抗旋转的力,并且血凝幅度(变量X)和血凝弹性(变量Y)之间的关系是非线性的。X的特定增量(ΔX)将与Y的不同增量(ΔY)相关,这取决于X的初始值。正确使用血凝弹性数据进行计算时,血凝块的血小板成分可以为紧急出血时的血小板缺乏情况提供有价值的见解。