Lui Michelle, Jones C Allyson, Westby Marie D
Department of Occupational Therapy, Surrey Memorial Hospital, 13750 96 Avenue, Surrey, BC, V3V 1Z2, Canada.
Department of Physical Therapy, University of Alberta, 8205 114 Street, 2-50 Corbett Hall, Edmonton, AB, T6G 2G4, Canada.
Syst Rev. 2015 Sep 27;4:121. doi: 10.1186/s13643-015-0107-2.
Of the more than 104,000 Canadians who underwent elective total joint arthroplasty (TJA) surgery in 2012-2013 for hip and knee osteoarthritis (OA), 40 and 60 %, respectively, were obese. Obesity is associated with increased risks for receiving TJA, post-operative complications and delayed functional recovery. Current guidelines for patients with a body mass index (BMI) of ≥30 kg/m(2) are to participate in a weight management programme and to lose weight prior to TJA surgery. As part of a larger project, a rapid review was conducted to examine the effects of short-term non-pharmacological and non-surgical weight loss interventions in adults in the year prior to total hip arthroplasty (THA) and total knee arthroplasty (TKA) on surgical and patient outcomes, and adverse events.
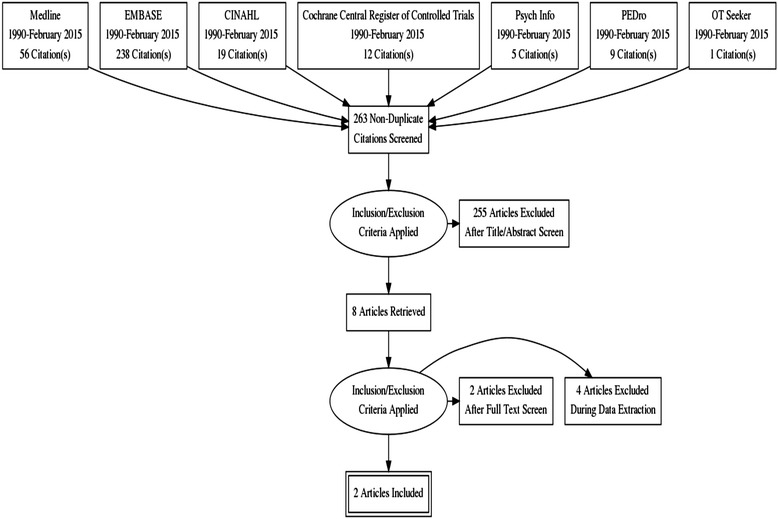
We performed a rapid review and searched seven electronic databases for English language articles published between 1990 and February 2015. Observational studies evaluating the association between pre-operative weight loss and short- and long-term outcomes, and controlled trials of non-pharmacological and non-surgical weight loss interventions were considered for inclusion. Two reviewers independently screened and selected articles, assessed methodological quality and extracted data.
Of 263 articles identified, a total of four studies met our inclusion criteria. In one of two high-quality retrospective cohort studies, weight loss ≥5 % of body weight in the year prior to TJA and maintained in the year after surgery was associated with a higher likelihood of deep surgical site infection in THA patients and 90-day readmission in TKA patients. No significant differences were reported in incidence of superficial surgical site infections in THA or TKA patients who lost weight pre-operatively compared to those who maintained their weight in either study. Two abstracts of randomized controlled trials were included; however, despite contacting the authors, full-length articles were not available. The limited information from the trials suggested that short-term dietician-supervised weight loss interventions were effective in weight loss prior to TJA.
There is limited evidence to support the recommendation of weight loss in the year prior to TJA and to determine the effectiveness of short-term non-pharmacological, non-surgical weight management interventions on patient and surgical outcomes.
在2012 - 2013年因髋膝关节骨关节炎(OA)接受择期全关节置换术(TJA)的104,000多名加拿大人中,分别有40%和60%的人肥胖。肥胖与接受TJA的风险增加、术后并发症以及功能恢复延迟有关。目前针对体重指数(BMI)≥30 kg/m²的患者的指南是参加体重管理计划并在TJA手术前减重。作为一个更大项目的一部分,我们进行了一项快速综述,以研究在全髋关节置换术(THA)和全膝关节置换术(TKA)前一年,成人短期非药物和非手术减重干预对手术和患者结局以及不良事件的影响。
我们进行了一项快速综述,并在七个电子数据库中检索了1990年至2015年2月发表的英文文章。纳入评估术前减重与短期和长期结局之间关联的观察性研究,以及非药物和非手术减重干预的对照试验。两名评审员独立筛选和选择文章、评估方法学质量并提取数据。
在识别出的263篇文章中,共有四项研究符合我们的纳入标准。在两项高质量回顾性队列研究中的一项中,TJA前一年体重减轻≥5%且术后一年保持该体重,与THA患者深部手术部位感染的可能性增加以及TKA患者90天再入院的可能性增加有关。在这两项研究中,术前减重的THA或TKA患者与体重保持不变的患者相比,浅表手术部位感染的发生率均未报告有显著差异。纳入了两项随机对照试验的摘要;然而,尽管与作者联系,但未获得全文。试验中的有限信息表明,短期由营养师监督的减重干预在TJA前减重方面是有效的。
支持在TJA前一年进行减重以及确定短期非药物、非手术体重管理干预对患者和手术结局有效性的证据有限。