Attri Joginder Pal, Kaur Gagandeep, Kaur Sarabjit, Kaur Ravneet, Mohan Brij, Kashyap Kamaljyoti
Department of Anaesthesia, Government Medical College, Amritsar, Punjab, India.
Anesth Essays Res. 2015 May-Aug;9(2):178-84. doi: 10.4103/0259-1162.152148.
Intrathecal opioids added to low dose local anesthetics in spinal anaesthesia intensifies sensory block without affecting sympathetic blockade. Aim was to evaluate the safety and efficacy of intrathecal levobupivacaine plain versus levobupivacaine plus fentanyl in infraumbilical surgeries.
In a prospective randomized double blind study, 100 patients of American Society of Anesthesiologists grades I and II of either sex, 20-65 years of age were included after approval from the Ethics Committee. Informed consent was taken and patients were randomly divided into two groups of 50 each, to receive either 2 ml of 0.5% isobaric levobupivacaine (group L) or 2 ml of 0.5% isobaric levobupivacaine + 25 μg fentanyl (group LF) intrathecally. Patients were monitored for sensory and motor block characteristics, postoperative analgesia, haemodynamics and side effects and complications for 24 h.
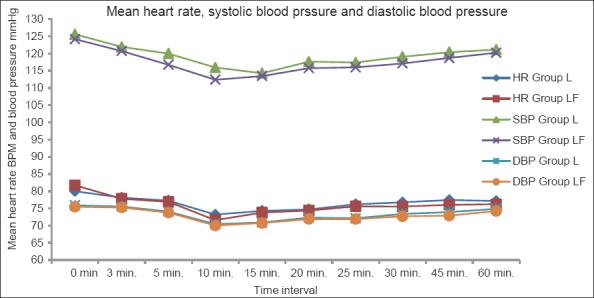
Onset of sensory block and time to maximum sensory block was rapid in group LF (4.8 ± 1.50 and 8.46 ± 1.87 min) as compared to group L (7.6 ± 1.46 and 15.80 ± 2.43 min) (P < 0.000). Maximum sensory block was T6 in group LF and T8 in group L. Maximum Bromage score was 2 in both groups but was achieved earlier in group LF (P < 0.000). Duration of sensory and motor block was significantly prolonged in group LF (270.98 ± 28.60 and 188.52 ± 9.81 min) as compared to group L (197.58 ± 11.20 and 152.76 ± 9.79 min). Total duration of analgesia was also prolonged in group LF (265.16 ± 26.18 min) as compared to group L (168.16 ± 11.08 min). Patients remained haemodynamically stable and side effects and complications were comparable in both groups. Data was analyzed using "Chi-square test" and "unpaired t-test."
Addition of fentanyl to levobupivacaine leads to early onset and prolonged duration of sensory and motor block as well as postoperative analgesia with stable haemodynamics and minimal side effects.
在脊髓麻醉中,鞘内注射阿片类药物与低剂量局部麻醉药联合使用可增强感觉阻滞,而不影响交感神经阻滞。目的是评估单纯鞘内注射左旋布比卡因与左旋布比卡因加芬太尼用于脐下手术的安全性和有效性。
在一项前瞻性随机双盲研究中,经伦理委员会批准,纳入100例年龄在20 - 65岁之间、美国麻醉医师协会分级为I级和II级的男女患者。获取知情同意后,将患者随机分为两组,每组50例,分别鞘内注射2 ml 0.5%等比重左旋布比卡因(L组)或2 ml 0.5%等比重左旋布比卡因 + 25 μg芬太尼(LF组)。对患者进行24小时的感觉和运动阻滞特征、术后镇痛、血流动力学以及副作用和并发症的监测。
与L组(7.6 ± 1.46和15.80 ± 2.43分钟)相比,LF组的感觉阻滞起效时间和达到最大感觉阻滞的时间更快(4.8 ± 1.50和8.46 ± 1.87分钟)(P < 0.000)。LF组的最大感觉阻滞平面为T6,L组为T8。两组的最大布罗麻评分均为2,但LF组更早达到(P < 0.000)。与L组(197.58 ± 11.20和152.76 ± 9.79分钟)相比,LF组的感觉和运动阻滞持续时间显著延长(270.98 ± 28.60和188.52 ± 9.81分钟)。LF组的总镇痛持续时间也比L组延长(265.16 ± 26.18分钟 vs 168.16 ± 11.08分钟)。患者血流动力学保持稳定,两组的副作用和并发症相当。数据采用“卡方检验”和“非配对t检验”进行分析。
左旋布比卡因中添加芬太尼可导致感觉和运动阻滞以及术后镇痛的起效提前和持续时间延长,同时血流动力学稳定,副作用最小。