Zhang Zhongheng, Chen Kun, Chen Lin
Department of critical care medicine, Jinhua municipal central hospital, Jinhua hospital of Zhejiang university, Zhejiang, P. R. China.
PLoS One. 2015 Sep 30;10(9):e0139374. doi: 10.1371/journal.pone.0139374. eCollection 2015.
Acute Physiology and Chronic Health Evaluation (APACHE) III score has been widely used for prediction of clinical outcomes in mixed critically ill patients. However, it has not been validated in patients with sepsis-associated acute lung injury (ALI). The aim of the study was to explore the calibration and predictive value of APACHE III in patients with sepsis-associated ALI.
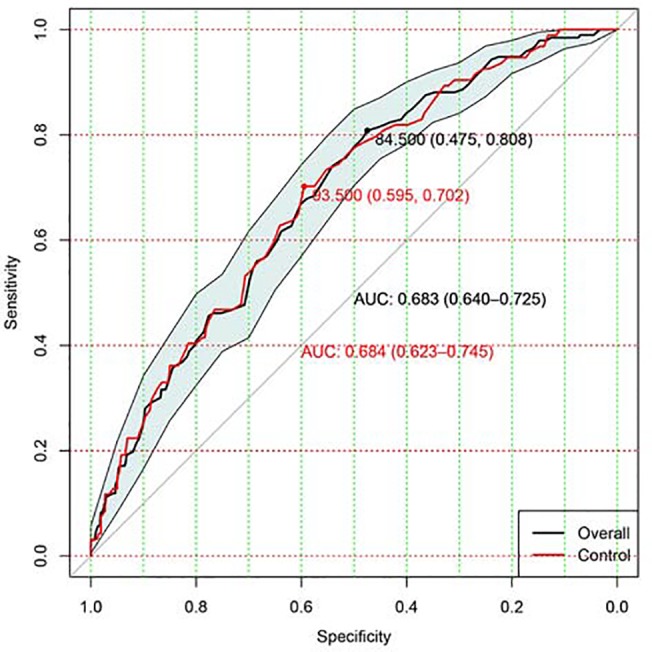
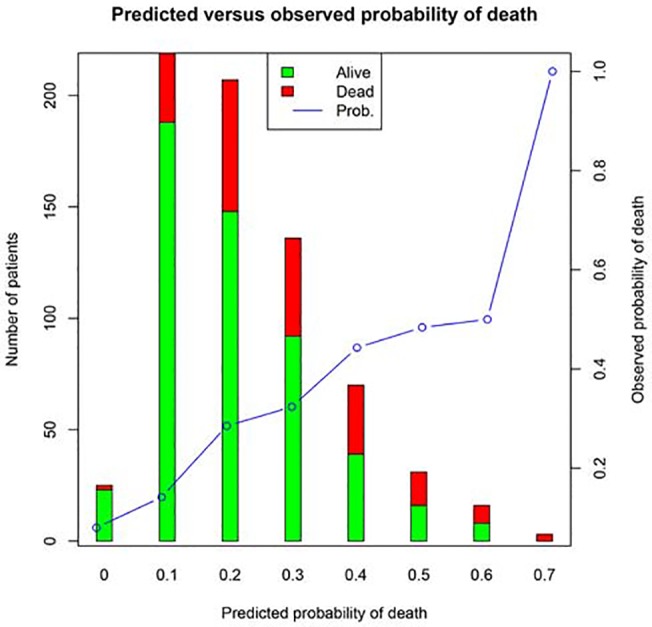
The study was a secondary analysis of a prospective randomized controlled trial investigating the efficacy of rosuvastatin in sepsis-associated ALI (Statins for Acutely Injured Lungs from Sepsis, SAILS). The study population was sepsis-related ALI patients. The primary outcome of the current study was the same as in the original trial, 60-day in-hospital mortality, defined as death before hospital discharge, censored 60 days after enrollment. Discrimination of APACHE III was assessed by calculating the area under the receiver operating characteristic (ROC) curve (AUC) with its 95% CI. Hosmer-Lemeshow goodness-of-fit statistic was used to assess the calibration of APACHE III. The Brier score was reported to represent the overall performance of APACHE III in predicting outcome.
A total of 745 patients were included in the study, including 540 survivors and 205 non-survivors. Non-survivors were significantly older than survivors (59.71 ± 16.17 vs 52.00 ± 15.92 years, p < 0.001). The primary causes of ALI were also different between survivors and non-survivors (p = 0.017). Survivors were more likely to have the cause of sepsis than non-survivors (21.2% vs. 15.1%). APACHE III score was higher in non-survivors than in survivors (106.72 ± 27.30 vs. 88.42 ± 26.86; p < 0.001). Discrimination of APACHE III to predict mortality in ALI patients was moderate with an AUC of 0.68 (95% confidence interval: 0.64-0.73).
this study for the first time validated the discrimination of APACHE III in sepsis associated ALI patients. The result shows that APACHE III score has moderate predictive value for in-hospital mortality among adults with sepsis-associated acute lung injury.
急性生理学与慢性健康状况评估(APACHE)Ⅲ评分已广泛用于预测危重症混合患者的临床结局。然而,其在脓毒症相关急性肺损伤(ALI)患者中尚未得到验证。本研究的目的是探讨APACHEⅢ在脓毒症相关ALI患者中的校准情况及预测价值。
本研究是一项前瞻性随机对照试验的二次分析,该试验旨在研究瑞舒伐他汀对脓毒症相关ALI的疗效(脓毒症所致急性肺损伤的他汀类药物治疗,SAILS)。研究人群为脓毒症相关ALI患者。本研究的主要结局与原试验相同,即60天院内死亡率,定义为出院前死亡,入组60天后进行截尾。通过计算受试者工作特征(ROC)曲线下面积(AUC)及其95%置信区间来评估APACHEⅢ的辨别力。采用Hosmer-Lemeshow拟合优度统计量来评估APACHEⅢ的校准情况。报告Brier评分以代表APACHEⅢ在预测结局方面的总体表现。
本研究共纳入745例患者,其中540例存活,205例未存活。未存活者的年龄显著高于存活者(59.71±16.17岁 vs 52.00±15.92岁;p<0.001)。存活者和未存活者ALI的主要病因也有所不同(p = 0.017)。存活者因脓毒症导致ALI的可能性高于未存活者(21.2%对15.1%)。未存活者的APACHEⅢ评分高于存活者(106.72±27.30对88.42±26.86;p<0.001)。APACHEⅢ预测ALI患者死亡率的辨别力中等,AUC为0.68(95%置信区间:0.64 - 0.73)。
本研究首次验证了APACHEⅢ在脓毒症相关ALI患者中的辨别力。结果表明,APACHEⅢ评分对脓毒症相关急性肺损伤成人患者的院内死亡率具有中等预测价值。