Wood Frances, Salam Abdul, Singh Kavita, Day Sophie, Jan Stephen, Prabhakaran Dorairaj, Rodgers Anthony, Patel Anushka, Thom Simon, Ward Helen
International Centre for Circulatory Health, Imperial College London and Imperial Healthcare NHS Trust, London, UK.
George Institute for Global Health, Hyderabad, Telangana, India The George Institute for Global Health, University of Sydney, Camperdown, New South Wales, Australia.
BMJ Open. 2015 Sep 30;5(9):e008018. doi: 10.1136/bmjopen-2015-008018.
The Use of a Multidrug Pill In Reducing cardiovascular Events (UMPIRE) trial has shown improved adherence with the use of a polypill strategy when compared with usual medications for cardiovascular disease (CVD) prevention. To advance from efficacy to impact, we need a better understanding of why and how such a strategy might be deployed in complex health systems.
To understand, from the perspective of UMPIRE trial participants and professionals, how and why a polypill strategy improves adherence compared with usual care, why improvement is greater in some subgroups, and to explore the acceptability of a polypill strategy among trial participants and healthcare professionals.
DESIGN, SETTING AND PARTICIPANTS: A preplanned process evaluation, based on qualitative interviews, was conducted with a subsample of 102 trial participants and 41 healthcare professionals at the end of the UMPIRE trial in India and Europe.
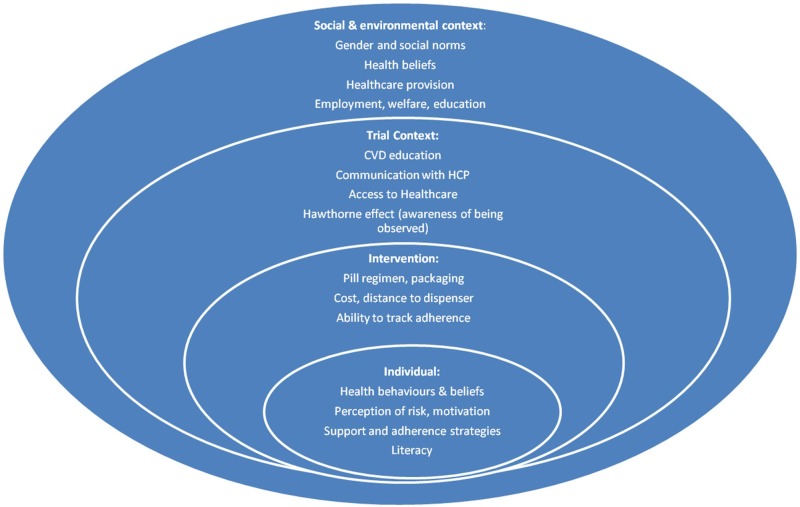
Most patients contrasted the simplicity of the polypill with usual medications that they found complex and, for many in India, expensive. Patients with low baseline adherence struggled most with complex medication lists, and those without established disease described less motivation to adhere when compared with people who had already been diagnosed with CVD; people in the latter group had already undertaken self-directed measures to adhere to CVD preventive medicines prior to entering the trial. Taking medication was one of many adaptations described by patients; these included dietary changes, stopping smoking and maintaining exercise. Most patients liked the polypill strategy, although some participants and health professionals were concerned that it would provide less tailored therapy for individual needs.
Adherence to treatment lists with multiple medications is complex and influenced by several factors. Simplifying medication by using a once-daily polypill is one approach to CVD prevention that may enhance adherence. Prescribers should also consider the wide variety of adjustments that individuals need to make to cope with daily medication.
与用于预防心血管疾病(CVD)的常规药物相比,多药复方药丸降低心血管事件(UMPIRE)试验表明,采用多药复方药丸策略可提高依从性。为了从疗效推进到影响,我们需要更好地理解为何以及如何在复杂的卫生系统中部署这样的策略。
从UMPIRE试验参与者和专业人员的角度,了解与常规护理相比,多药复方药丸策略如何以及为何能提高依从性,为何在某些亚组中改善更大,并探讨多药复方药丸策略在试验参与者和医疗保健专业人员中的可接受性。
设计、设置和参与者:在印度和欧洲的UMPIRE试验结束时,对102名试验参与者和41名医疗保健专业人员的子样本进行了基于定性访谈的预先计划的过程评估。
大多数患者将多药复方药丸的简单性与他们认为复杂且对许多印度患者来说昂贵的常规药物进行了对比。基线依从性低的患者在面对复杂的药物清单时最为困难,与已被诊断患有CVD的人相比,未确诊疾病的人描述的依从动机较低;后一组人在进入试验之前已经采取了自我指导措施来坚持服用CVD预防药物。服药是患者描述的多种调整之一;这些调整包括饮食改变、戒烟和坚持锻炼。大多数患者喜欢多药复方药丸策略,尽管一些参与者和卫生专业人员担心它不能根据个体需求提供更个性化的治疗。
坚持服用多种药物的治疗清单很复杂,且受多种因素影响。通过使用每日一次的多药复方药丸简化用药是预防CVD的一种方法,可能会提高依从性。开处方者还应考虑个体为应对日常用药需要进行的各种调整。