Stanford Prevention Research Center, Stanford University, Stanford, CA, USA.
School of Population and Public Health, University of British Columbia, Vancouver, BC, Canada.
Lancet HIV. 2014 Dec;1(3):e104-11. doi: 10.1016/S2352-3018(14)00003-4. Epub 2014 Nov 24.
Adherence to antiretroviral therapy (ART) is necessary for the improvement of the health of patients and for public health. We sought to determine the comparative effectiveness of different interventions for improving ART adherence in HIV-infected people living in Africa.
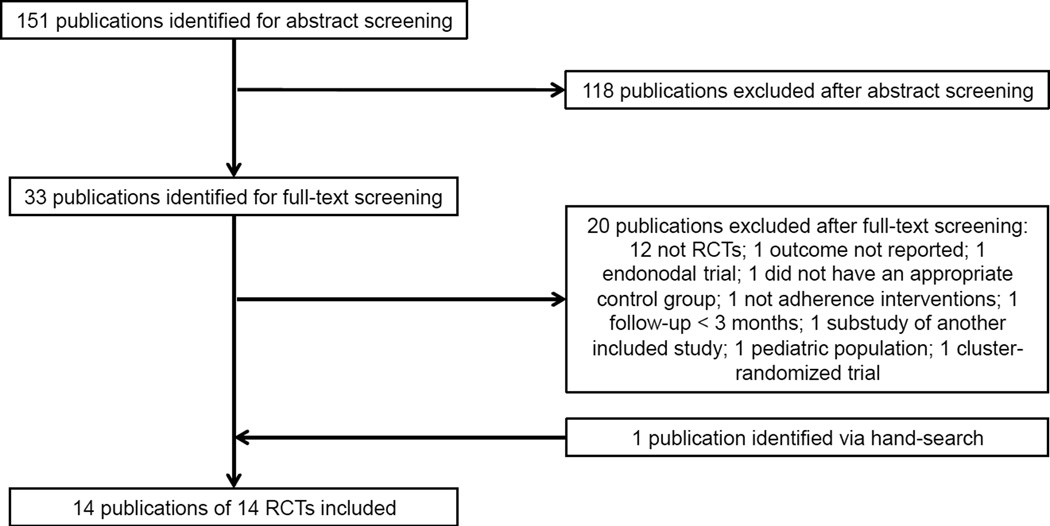
We searched for randomised trials of interventions to promote antiretroviral adherence within adults in Africa. We searched AMED, CINAHL, Embase, Medline (via PubMed), and ClinicalTrials.gov from inception to Oct 31, 2014, with the terms "HIV", "ART", "adherence", and "Africa". We created a network of the interventions by pooling the published and individual patients' data for comparable treatments and comparing them across the individual interventions with Bayesian network meta-analyses. The primary outcome was adherence defined as the proportion of patients meeting trial defined criteria; the secondary endpoint was viral suppression.
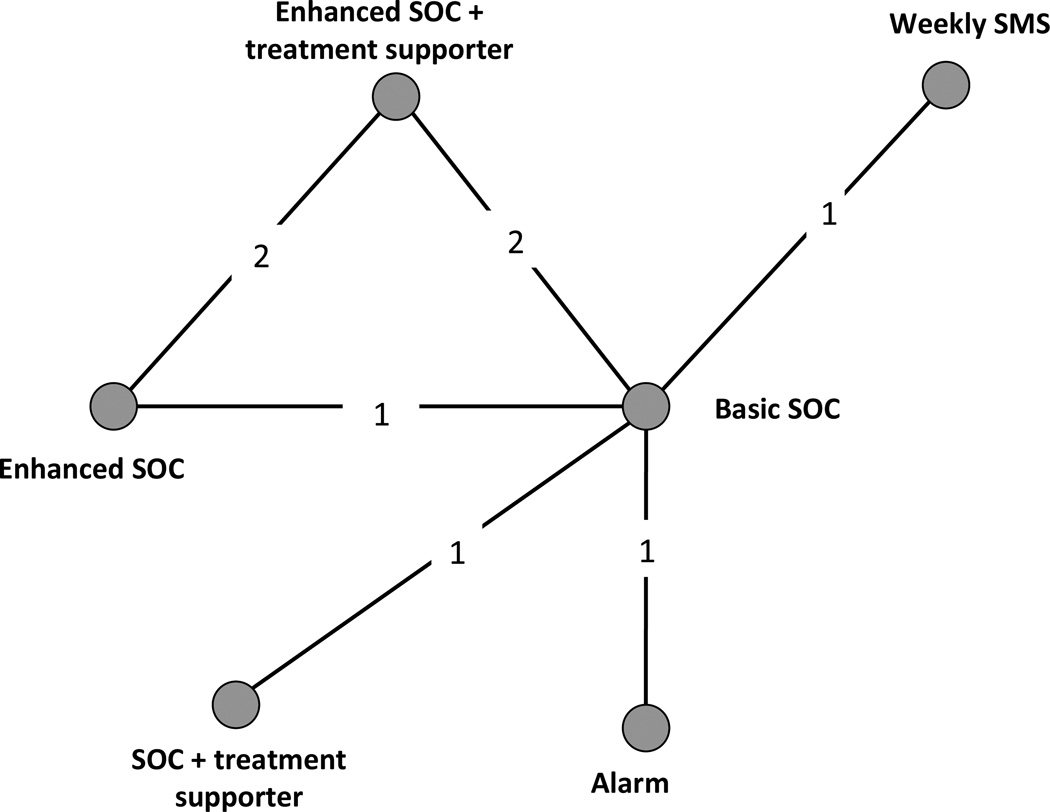
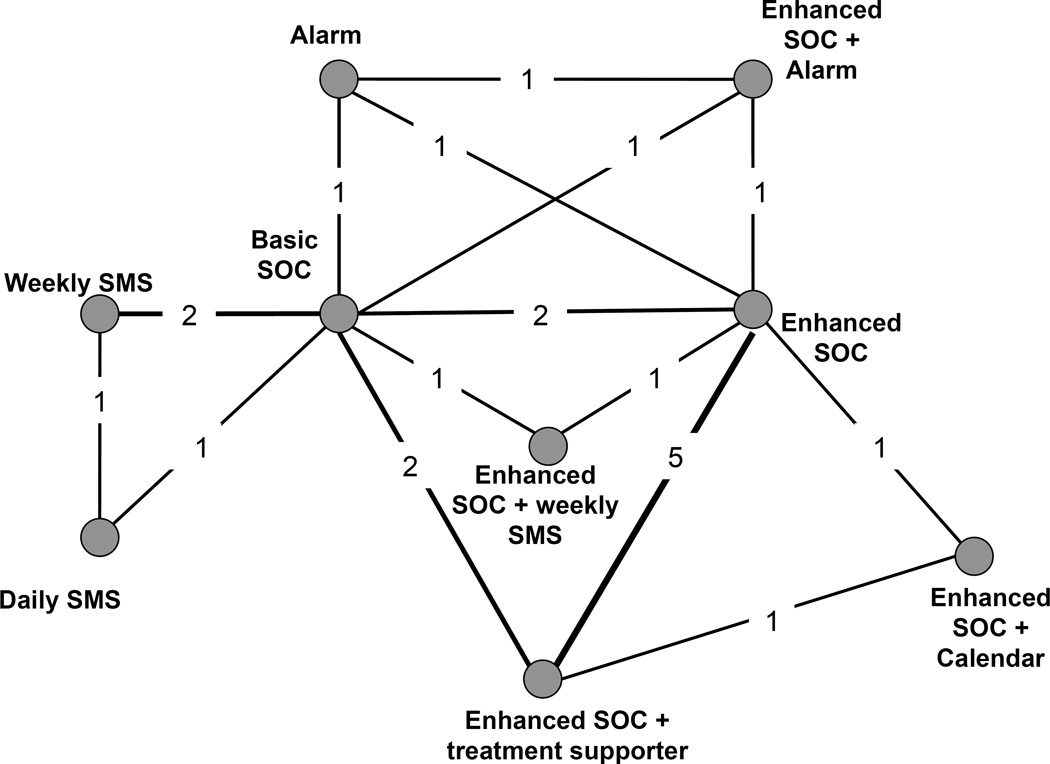
We obtained data for 14 randomised controlled trials, with 7110 patients. Interventions included daily and weekly short message service (SMS; text message) messaging, calendars, peer supporters, alarms, counselling, and basic and enhanced standard of care (SOC). Compared with SOC, we found distinguishable improvement in self-reported adherence with enhanced SOC (odds ratio [OR] 1·46, 95% credibility interval [CrI] 1·06-1·98), weekly SMS messages (1·65, 1·25-2·18), counselling and SMS combined (2·07, 1·22-3·53), and treatment supporters (1·83, 1·36-2·45). We found no compelling evidence for the remaining interventions. Results were similar when using viral suppression as an outcome, although the network contained less evidence than that for adherence. Treatment supporters with enhanced SOC (1·46, 1·09-1·97) and weekly SMS messages (1·55, 1·01-2·38) were significantly better than basic SOC.
Several recommendations for improving adherence are unsupported by the available evidence. These findings can inform future intervention choices for improving ART adherence in low-income settings.
None.
抗逆转录病毒疗法(ART)的依从性对于改善患者健康和公共卫生至关重要。我们旨在确定不同干预措施在提高非洲艾滋病毒感染者接受 ART 治疗的依从性方面的比较效果。
我们在非洲成年人中搜索了促进抗逆转录病毒依从性的随机试验。我们于 2014 年 10 月 31 日之前在 AMED、CINAHL、Embase、Medline(通过 PubMed)和 ClinicalTrials.gov 中搜索了术语“HIV”、“ART”、“依从性”和“非洲”的干预措施。我们通过汇集已发表和个体患者的数据,对可比较的治疗方法进行了网络构建,并对每个干预措施进行了贝叶斯网络荟萃分析,从而对干预措施进行了网络构建。主要结局是定义为符合试验定义标准的患者比例的依从性;次要终点是病毒抑制。
我们获得了 14 项随机对照试验的数据,涉及 7110 名患者。干预措施包括每日和每周短消息服务(SMS;短信)消息传递、日历、同伴支持者、警报、咨询以及基本和增强的标准护理(SOC)。与 SOC 相比,我们发现增强 SOC(比值比[OR]1·46,95%可信区间[CrI]1·06-1·98)、每周 SMS 消息(1·65,1·25-2·18)、咨询和 SMS 相结合(2·07,1·22-3·53)以及治疗支持者(1·83,1·36-2·45)在自我报告的依从性方面有明显改善。对于其余的干预措施,我们没有发现令人信服的证据。当使用病毒抑制作为结果时,结果相似,尽管网络中包含的证据少于依从性的证据。增强 SOC 的治疗支持者(1·46,1·09-1·97)和每周 SMS 消息(1·55,1·01-2·38)明显优于基本 SOC。
一些改善依从性的建议没有得到现有证据的支持。这些发现可以为改善低收入环境下 ART 依从性的未来干预措施选择提供信息。
无。