Kahn Jeremy M, Barnato Amber E, Lave Judith R, Pike Francis, Weissfeld Lisa A, Le Tri Q, Angus Derek C
Clinical Research, Investigation and Systems Modeling of Acute Illness (CRISMA) Center, Department of Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, United States of America; Department of Health Policy & Management, University of Pittsburgh Graduate School of Public Health, Pittsburgh, Pennsylvania, United States of America.
Clinical Research, Investigation and Systems Modeling of Acute Illness (CRISMA) Center, Department of Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, United States of America; Department of Health Policy & Management, University of Pittsburgh Graduate School of Public Health, Pittsburgh, Pennsylvania, United States of America; Center for Research on Health Care, Division of General Internal Medicine, University of Pittsburgh School of Medicine, Pittsburgh Pennsylvania, United States of America.
PLoS One. 2015 Oct 6;10(10):e0139742. doi: 10.1371/journal.pone.0139742. eCollection 2015.
Long-term acute care hospitals (LTACs) provide specialized treatment for patients with chronic critical illness. Increasingly LTACs are co-located within traditional short-stay hospitals rather than operated as free-standing facilities, which may affect LTAC utilization patterns and outcomes.
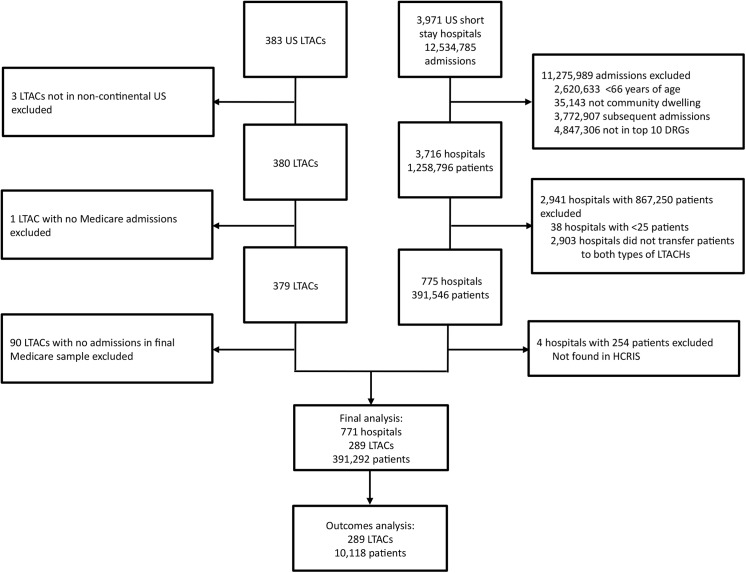
We compared free-standing and co-located LTACs using 2005 data from the United States Centers for Medicare & Medicaid Services. We used bivariate analyses to examine patient characteristics and timing of LTAC transfer, and used propensity matching and multivariable regression to examine mortality, readmissions, and costs after transfer.
Of 379 LTACs in our sample, 192 (50.7%) were free-standing and 187 (49.3%) were co-located in a short-stay hospital. Co-located LTACs were smaller (median bed size: 34 vs. 66, p <0.001) and more likely to be for-profit (72.2% v. 68.8%, p = 0.001) than freestanding LTACs. Co-located LTACs admitted patients later in their hospital course (average time prior to transfer: 15.5 days vs. 14.0 days) and were more likely to admit patients for ventilator weaning (15.9% vs. 12.4%). In the multivariate propensity-matched analysis, patients in co-located LTACs experienced higher 180-day mortality (adjusted relative risk: 1.05, 95% CI: 1.00-1.11, p = 0.04) but lower readmission rates (adjusted relative risk: 0.86, 95% CI: 0.75-0.98, p = 0.02). Costs were similar between the two hospital types (mean difference in costs within 180 days of transfer: -$3,580, 95% CI: -$8,720 -$1,550, p = 0.17).
Compared to patients in free-standing LTACs, patients in co-located LTACs experience slightly higher mortality but lower readmission rates, with no change in overall resource use as measured by 180 day costs.
长期急性病医院(LTACs)为慢性危重病患者提供专门治疗。越来越多的长期急性病医院与传统的短期住院医院设在同一地点,而不是作为独立设施运营,这可能会影响长期急性病医院的利用模式和治疗效果。
我们使用美国医疗保险和医疗补助服务中心2005年的数据,对独立的长期急性病医院和设在同一地点的长期急性病医院进行了比较。我们使用双变量分析来检查患者特征和长期急性病医院的转诊时间,并使用倾向匹配和多变量回归来检查转诊后的死亡率、再入院率和费用。
在我们的样本中的379家长期急性病医院中,192家(50.7%)是独立的,187家(49.3%)与短期住院医院设在同一地点。与独立的长期急性病医院相比,设在同一地点的长期急性病医院规模较小(中位数床位规模:34张对66张,p<0.001),且更有可能是营利性的(72.2%对68.8%,p = 0.001)。设在同一地点的长期急性病医院在患者住院过程中较晚收治患者(转诊前平均时间:15.5天对14.0天),且更有可能收治需要撤机的患者(15.9%对12.4%)。在多变量倾向匹配分析中,设在同一地点的长期急性病医院的患者180天死亡率较高(调整后的相对风险:1.05,95%可信区间:1.00 - 1.11,p = 0.04),但再入院率较低(调整后的相对风险:0.86,95%可信区间:0.75 - 0.98,p = 0.02)。两种医院类型的费用相似(转诊后180天内费用的平均差异:-3580美元,95%可信区间:-8720美元至-1550美元,p = 0.17)。
与独立的长期急性病医院的患者相比,设在同一地点的长期急性病医院的患者死亡率略高,但再入院率较低,以180天费用衡量的总体资源使用情况没有变化。