Baikoussis Nikolaos G, Papakonstantinou Nikolaos A, Verra Chrysoula, Kakouris Georgios, Chounti Maria, Hountis Panagiotis, Dedeilias Panagiotis, Argiriou Michalis
Department of Cardiovascular and Thoracic Surgery, "Evangelismos'' General Hospital of Athens, Athens, Greece.
Ann Card Anaesth. 2015 Oct-Dec;18(4):555-64. doi: 10.4103/0971-9784.166465.
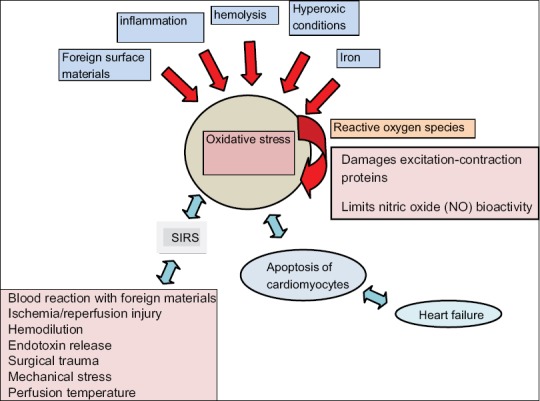
Cold heart protection via cardioplegia administration, limits the amount of oxygen demand. Systemic normothermia with warm cardioplegia was introduced due to the abundance of detrimental effects of hypothermia. A temperature of 32-33°C in combination with tepid blood cardioplegia of the same temperature appears to be protective enough for both; heart and brain. Reduction of nitric oxide (NO) concentration is in part responsible for myocardial injury after the cardioplegic cardiac arrest. Restoration of NO balance with exogenous NO supplementation has been shown useful to prevent inflammation and apoptosis. In this article, we discuss the "deleterious" effects of the oxidative stress of the extracorporeal circulation and the up-to-date theories of "ideal'' myocardial protection.
通过给予心脏停搏液进行心脏冷保护,可限制氧需求量。由于低温存在大量有害影响,因此引入了全身常温与温血心脏停搏液相结合的方法。32 - 33°C的温度与相同温度的微温血心脏停搏液相结合,似乎对心脏和大脑都具有足够的保护作用。一氧化氮(NO)浓度的降低部分导致了心脏停搏后心肌损伤。已证明通过外源性补充NO来恢复NO平衡有助于预防炎症和细胞凋亡。在本文中,我们讨论体外循环氧化应激的“有害”影响以及“理想”心肌保护的最新理论。