Fischer Anja, Fischer Marcus, Nicholls Robert A, Lau Stephanie, Poettgen Jana, Patas Kostas, Heesen Christoph, Gold Stefan M
Department of Health Psychology, King's College London SE1 9RT, London, UK ; Center for Molecular Neurobiology, Institute of Neuroimmunology and Multiple Sclerosis (INIMS), University Medical Center Hamburg-Eppendorf Hamburg, Germany.
Department of Pharmaceutical Chemistry, University of California San Francisco San Francisco, California, 94158.
Brain Behav. 2015 Sep;5(9):e00365. doi: 10.1002/brb3.365. Epub 2015 Jul 14.
Multiple sclerosis and major depressive disorder frequently co-occur but depression often remains undiagnosed in this population. Self-rated depression questionnaires are a good option where clinician-based standardized diagnostics are not feasible. However, there is a paucity of data on diagnostic accuracy of self-report measures for depression in multiple sclerosis (MS). Moreover, head-to-head comparisons of common questionnaires are largely lacking. This could be particularly relevant for high-risk patients with depressive symptoms. Here, we compare the diagnostic accuracy of the Beck Depression Inventory (BDI) and 30-item version of the Inventory of Depressive Symptomatology Self-Rated (IDS-SR30) for major depressive disorder (MSS) against diagnosis by a structured clinical interview.
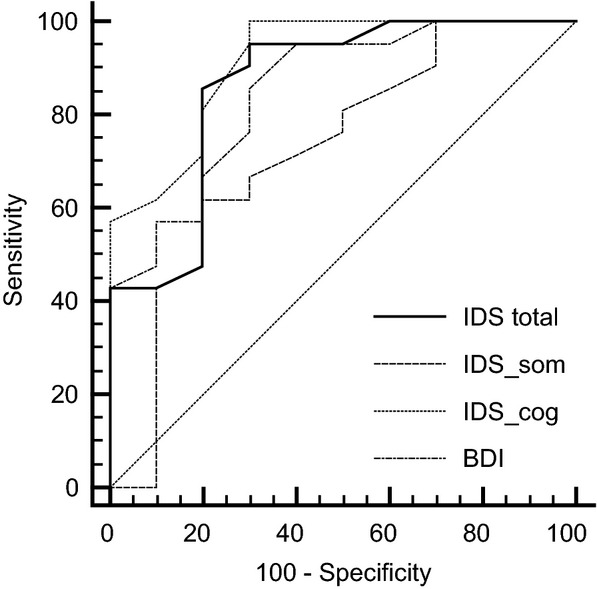
Patients reporting depressive symptoms completed the BDI, the IDS-SR30 and underwent diagnostic assessment (Mini International Neuropsychiatric Interview, M.I.N.I.). Receiver-Operating Characteristic analyses were performed, providing error estimates and false-positive/negative rates of suggested thresholds.
Data from n = 31 MS patients were available. BDI and IDS-SR30 total score were significantly correlated (r = 0.82). The IDS-SR30total score, cognitive subscore, and BDI showed excellent to good accuracy (area under the curve (AUC) 0.86, 0.91, and 0.85, respectively).
Both the IDS-SR30 and the BDI are useful to quantify depressive symptoms showing good sensitivity and specificity. The IDS-SR30 cognitive subscale may be useful as a screening tool and to quantify affective/cognitive depressive symptomatology.
多发性硬化症与重度抑郁症常同时出现,但该人群中的抑郁症往往未被诊断出来。在基于临床医生的标准化诊断不可行的情况下,自评抑郁问卷是一个不错的选择。然而,关于多发性硬化症(MS)中抑郁自评量表诊断准确性的数据很少。此外,常见问卷的直接比较在很大程度上也缺乏。这对于有抑郁症状的高危患者可能尤为重要。在此,我们将贝克抑郁量表(BDI)和抑郁症状自评量表30项版(IDS-SR30)针对重度抑郁症(MSS)的诊断准确性与结构化临床访谈的诊断结果进行比较。
报告有抑郁症状的患者完成BDI、IDS-SR30并接受诊断评估(迷你国际神经精神访谈,M.I.N.I.)。进行了受试者操作特征分析,提供了错误估计以及建议阈值的假阳性/阴性率。
有n = 31名MS患者的数据可用。BDI和IDS-SR30总分显著相关(r = 0.82)。IDS-SR30总分、认知子量表和BDI显示出极好到良好的准确性(曲线下面积(AUC)分别为0.86、0.91和0.85)。
IDS-SR30和BDI都有助于量化抑郁症状,显示出良好的敏感性和特异性。IDS-SR30认知子量表可用作筛查工具并量化情感/认知抑郁症状。