Tanaka Koji, Yamada Takeshi, Torii Takako, Yoshimura Takeo, Takase Kei-ichiro, Togao Osamu, Wakata Yoshifumi, Hiwatashi Akio, Nakashima Naoki, Kira Jun-ichi, Murai Hiroyuki
Department of Neurology, Neurological Institute, Graduate School of Medical Sciences, Kyushu University, 3-1-1 Maidashi, Higashi-ku, Fukuoka, 812-8582, Japan.
Department of Neurology, Saiseikai Fukuoka General Hospital, 1-3-46 Tenjin, Chuo-ku, Fukuoka, 810-0001, Japan.
BMC Neurol. 2015 Oct 7;15:184. doi: 10.1186/s12883-015-0439-5.
Pure dysarthria (PD) and dysarthria-facial paresis syndrome (DFP) mainly result from lenticulostriate artery territory infarction. PD and DFP are rare clinical entities, often grouped without distinction. The purpose of this study was to examine clinical and radiographic differences between PD and DFP due to unilateral internal capsule and/or corona radiata infarction.
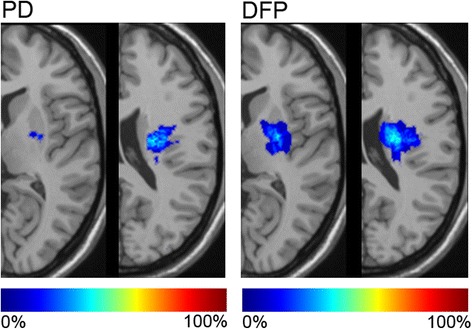
Using a database that included consecutive patients with ischemic stroke admitted to the neurological stroke units of three hospitals within 7 days from onset between September 2011 and April 2014, we retrospectively extracted first-ever stroke patient data, who presented with PD or DFP with a single ischemic lesion localized in the internal capsule and/or corona radiata. Patients with weakness, ataxia, sensory deficit, or cortical symptoms were excluded. Ischemic lesion volume was calculated by the ABC/2 method on diffusion-weighted imaging (DWI). DWI images were normalized and superimposed to the template for PD and DFP. We compared patients' characteristics between PD and DFP.
A total of 2126 patients, including 65 patients (3.1%) with PD or DFP, were registered. Of these, 13 PD patients and 18 patients with DFP due to unilateral internal capsule and/or corona radiata infarction were included for analysis. Compared with DFP patients, PD patients had longer onset-to-door time (median 37.5 vs. 10.8 h, p = 0.031), shorter vertical length (C component) of ischemic lesions (median 12.0 vs. 18.8 mm, p = 0.007), and smaller ischemic lesion volume (median 285 vs. 828 mm(3), p = 0.023). Ischemic lesions causing PD were located more frequently in the left hemisphere than DFP (92% vs. 56%, p = 0.045). The superimposed lesion pattern indicated that DFP had lesions more medial and involving posterior portions of the putamen and the caudate body, as well as more of the genu and posterior limb of the internal capsule, than PD. Ninety days after onset, symptoms disappeared in 21 (72%) out of 29 patients.
In cerebral infarction limited to the internal capsule and/or corona radiata, PD is derived from smaller and left-sided lesions with delay in diagnosis compared with DFP. The clinical course of those with PD and DFP might be benign.
纯构音障碍(PD)和构音障碍-面瘫综合征(DFP)主要由豆纹动脉供血区梗死引起。PD和DFP是罕见的临床病症,常被不加区分地归为一类。本研究的目的是探讨单侧内囊和/或放射冠梗死所致PD和DFP之间的临床和影像学差异。
利用一个数据库,该数据库纳入了2011年9月至2014年4月期间发病7天内入住三家医院神经科卒中单元的连续缺血性卒中患者,我们回顾性提取了首次发生卒中且表现为PD或DFP、单个缺血性病灶局限于内囊和/或放射冠的患者数据。排除有肌无力、共济失调、感觉障碍或皮质症状的患者。通过扩散加权成像(DWI)上的ABC/2法计算缺血性病灶体积。对DWI图像进行标准化处理并叠加到PD和DFP的模板上。我们比较了PD和DFP患者的特征。
共登记了2126例患者,其中包括65例(3.1%)患有PD或DFP的患者。其中,纳入13例因单侧内囊和/或放射冠梗死导致的PD患者和18例DFP患者进行分析。与DFP患者相比,PD患者的起病至入院时间更长(中位数37.5小时对10.8小时,p = 0.031),缺血性病灶的垂直长度(C成分)更短(中位数12.0毫米对18.8毫米,p = 0.007),缺血性病灶体积更小(中位数285立方毫米对828立方毫米,p = 0.023)。导致PD的缺血性病灶比DFP更频繁地位于左半球(92%对56%,p = 0.045)。叠加的病灶模式表明,与PD相比,DFP的病灶更靠近内侧,累及壳核和尾状核的后部,以及更多的内囊膝部和后肢。发病90天后,29例患者中有21例(72%)症状消失。
在仅限于内囊和/或放射冠的脑梗死中,与DFP相比,PD源于较小的左侧病灶且诊断延迟。PD和DFP患者的临床病程可能是良性的。