Scher Howard I, Solo Kirk, Valant Jason, Todd Mary B, Mehra Maneesha
Genitourinary Oncology Service, Department of Medicine, Sidney Kimmel Center for Prostate and Urologic Cancers, Memorial Sloan Kettering Cancer Center, and Department of Medicine, Weill Cornell Medical College, New York, New York, United States of America.
Lexidyne, Colorado Springs, Colorado, United States of America.
PLoS One. 2015 Oct 13;10(10):e0139440. doi: 10.1371/journal.pone.0139440. eCollection 2015.
To identify patient populations most in need of treatment across the prostate cancer disease continuum, we developed a novel dynamic transition model based on risk of disease progression and mortality.
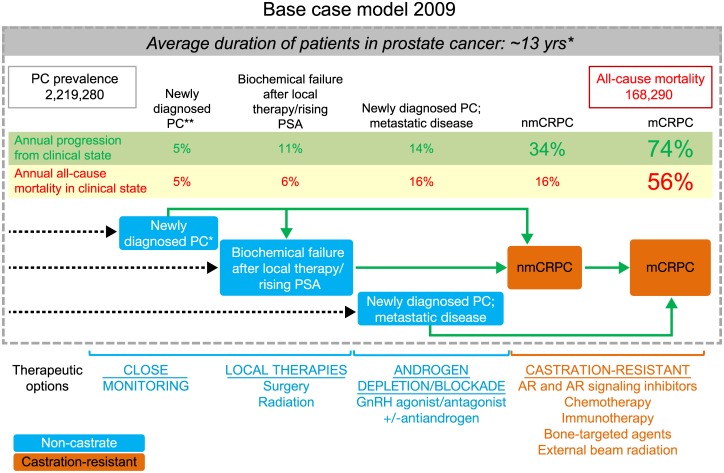
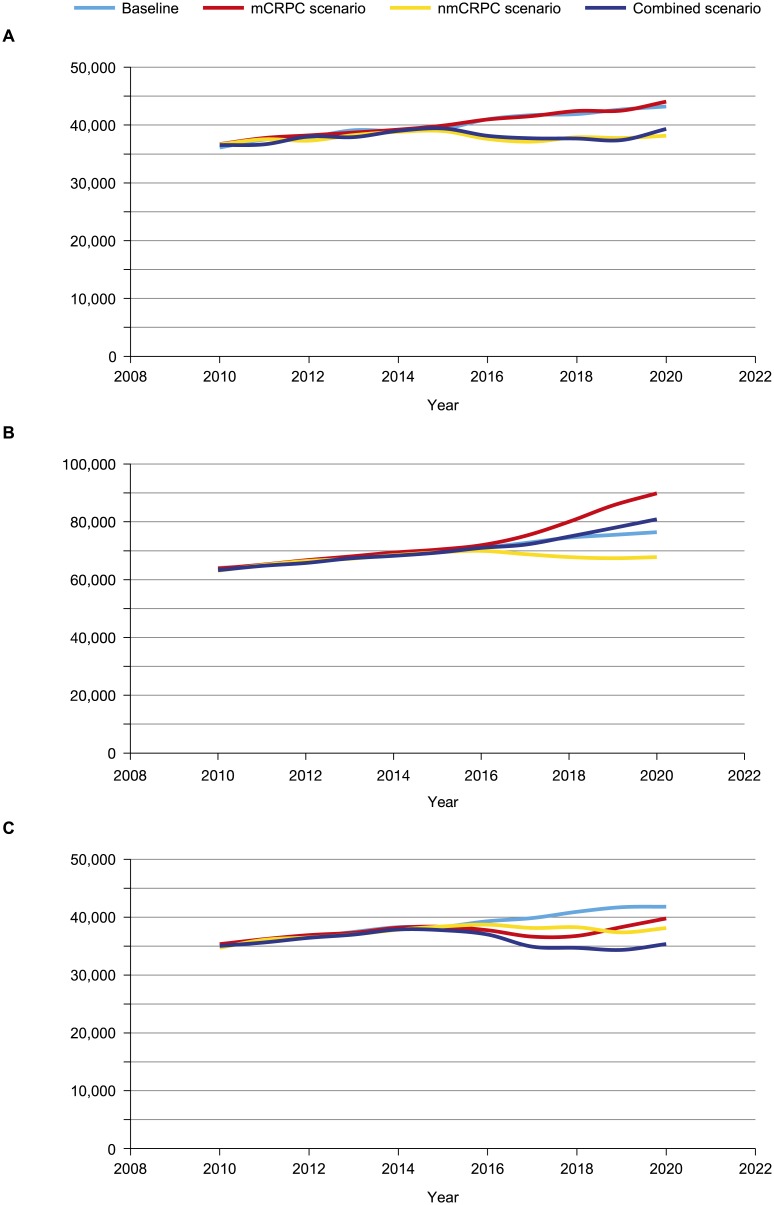
We modeled the flow of patient populations through eight prostate cancer clinical states (PCCS) that are characterized by the status of the primary tumor, presence of metastases, prior and current treatment, and testosterone levels. Simulations used published US incidence rates for each year from 1990. Progression and mortality rates were derived from published clinical trials, meta-analyses, and observational studies. Model outputs included the incidence, prevalence, and mortality for each PCCS. The impact of novel treatments was modeled in three distinct scenarios: metastatic castration-resistant prostate cancer (mCRPC), non-metastatic CRPC (nmCRPC), or both.
The model estimated the prevalence of prostate cancer as 2,219,280 in the US in 2009 and 3,072,480 in 2020, and incidence of mCRPC as 36,100 and 42,970, respectively. All-cause mortality in prostate cancer was estimated at 168,290 in 2009 and 219,360 in 2020, with 20.5% and 19.5% of these deaths, respectively, occurring in men with mCRPC. The majority (86%) of incidence flow into mCRPC states was from the nmCRPC clinical state. In the scenario with novel interventions for nmCRPC states, the progression to mCRPC is reduced, thus decreasing mCRPC incidence by 12% in 2020, with a sustained decline in mCRPC mortality. A limitation of the model is that it does not estimate prostate cancer-specific mortality.
The model informs clinical trial design for prostate cancer by quantifying outcomes in PCCS, and demonstrates the impact of an effective therapy applied in an earlier clinical state of nmCRPC on the incidence of mCRPC morbidity and subsequent mortality.
为了确定在前列腺癌疾病连续过程中最需要治疗的患者群体,我们基于疾病进展和死亡风险开发了一种新型动态转变模型。
我们对患者群体在八种前列腺癌临床状态(PCCS)中的流动情况进行了建模,这些状态由原发肿瘤状态、转移情况、既往和当前治疗以及睾酮水平来表征。模拟使用了1990年以来美国每年公布的发病率。进展率和死亡率来自已发表的临床试验、荟萃分析和观察性研究。模型输出包括每种PCCS的发病率、患病率和死亡率。在三种不同情况下对新型治疗的影响进行了建模:转移性去势抵抗性前列腺癌(mCRPC)、非转移性CRPC(nmCRPC)或两者都有。
该模型估计2009年美国前列腺癌患病率为2219280例,2020年为3072480例,mCRPC发病率分别为36100例和42970例。估计2009年前列腺癌全因死亡率为168290例,2020年为219360例,其中分别有20.5%和19.5%的死亡发生在mCRPC男性患者中。流入mCRPC状态的发病率大部分(86%)来自nmCRPC临床状态。在对nmCRPC状态进行新型干预的情况下,向mCRPC的进展减少,从而使2020年mCRPC发病率降低12%,mCRPC死亡率持续下降。该模型的一个局限性是它没有估计前列腺癌特异性死亡率。
该模型通过量化PCCS中的结果为前列腺癌临床试验设计提供信息,并证明了在nmCRPC的早期临床状态应用有效治疗对mCRPC发病率和随后死亡率的影响。