McKinlay Christopher J D, Alsweiler Jane M, Ansell Judith M, Anstice Nicola S, Chase J Geoffrey, Gamble Gregory D, Harris Deborah L, Jacobs Robert J, Jiang Yannan, Paudel Nabin, Signal Matthew, Thompson Benjamin, Wouldes Trecia A, Yu Tzu-Ying, Harding Jane E
From the Liggins Institute (C.J.D.M., J.M. Alsweiler, J.M. Ansell, G.D.G., D.L.H., Y.J., J.E.H.), the Department of Paediatrics (J.M. Alsweiler), the School of Optometry and Vision Science (N.S.A., R.J.J., N.P., B.T., T.-Y.Y.), and the Department of Psychological Medicine (T.A.W.), University of Auckland, Auckland, the Department of Mechanical Engineering, University of Canterbury, Christchurch (J.G.C., M.S.), and the Neonatal Intensive Care Unit, Waikato District Health Board, Hamilton (D.L.H.) - all in New Zealand; and the School of Optometry and Vision Science, University of Waterloo, Waterloo, ON, Canada (B.T.).
N Engl J Med. 2015 Oct 15;373(16):1507-18. doi: 10.1056/NEJMoa1504909.
Neonatal hypoglycemia is common and can cause neurologic impairment, but evidence supporting thresholds for intervention is limited.
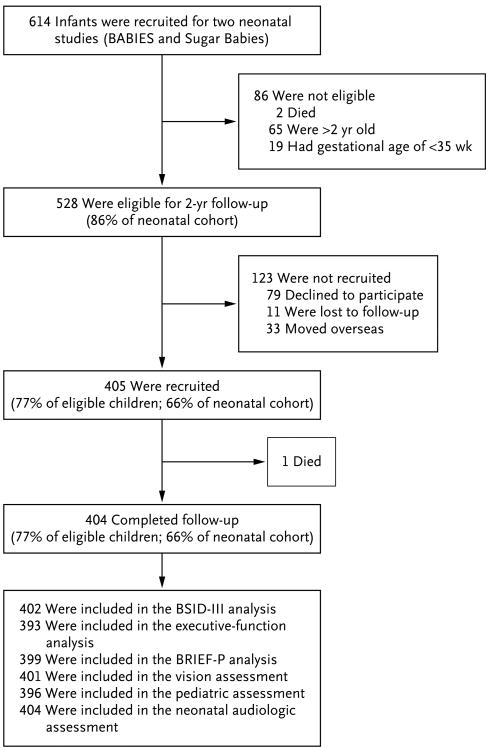
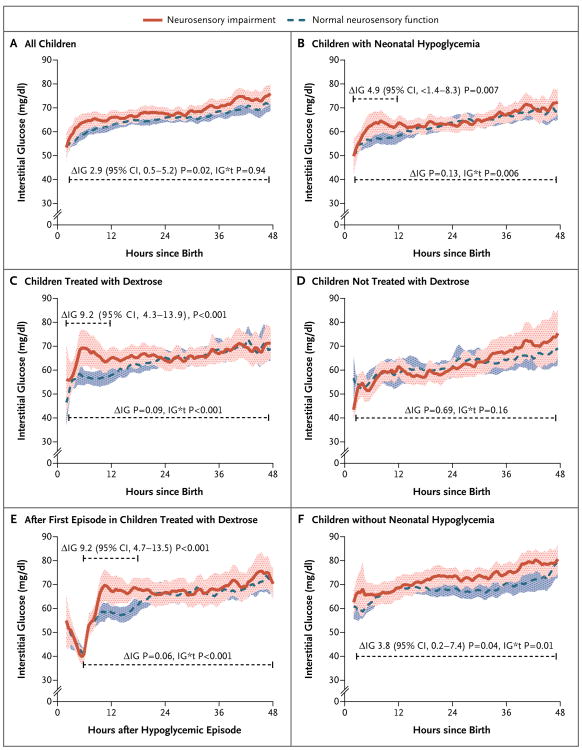
We performed a prospective cohort study involving 528 neonates with a gestational age of at least 35 weeks who were considered to be at risk for hypoglycemia; all were treated to maintain a blood glucose concentration of at least 47 mg per deciliter (2.6 mmol per liter). We intermittently measured blood glucose for up to 7 days. We continuously monitored interstitial glucose concentrations, which were masked to clinical staff. Assessment at 2 years included Bayley Scales of Infant Development III and tests of executive and visual function.
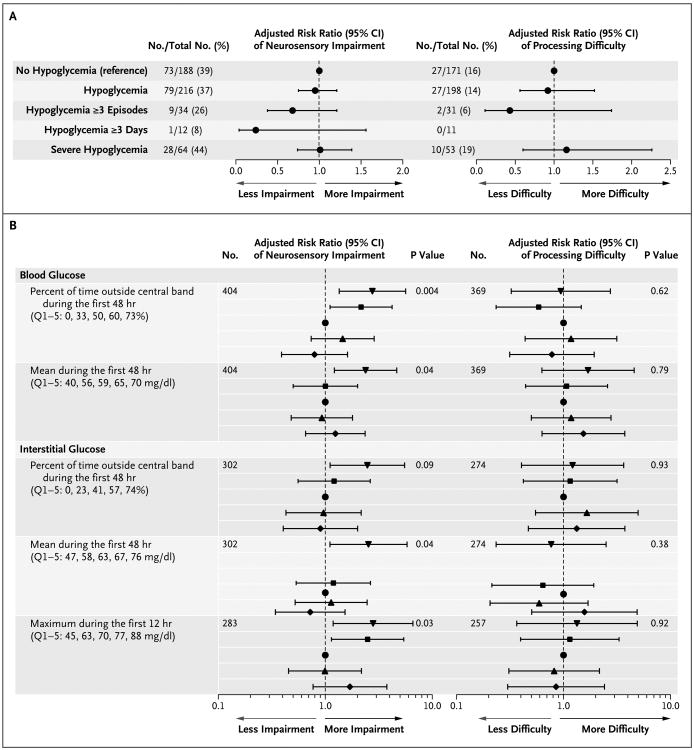
Of 614 children, 528 were eligible, and 404 (77% of eligible children) were assessed; 216 children (53%) had neonatal hypoglycemia (blood glucose concentration, <47 mg per deciliter). Hypoglycemia, when treated to maintain a blood glucose concentration of at least 47 mg per deciliter, was not associated with an increased risk of the primary outcomes of neurosensory impairment (risk ratio, 0.95; 95% confidence interval [CI], 0.75 to 1.20; P=0.67) and processing difficulty, defined as an executive-function score or motion coherence threshold that was more than 1.5 SD from the mean (risk ratio, 0.92; 95% CI, 0.56 to 1.51; P=0.74). Risks were not increased among children with unrecognized hypoglycemia (a low interstitial glucose concentration only). The lowest blood glucose concentration, number of hypoglycemic episodes and events, and negative interstitial increment (area above the interstitial glucose concentration curve and below 47 mg per deciliter) also did not predict the outcome.
In this cohort, neonatal hypoglycemia was not associated with an adverse neurologic outcome when treatment was provided to maintain a blood glucose concentration of at least 47 mg per deciliter. (Funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and others.).
新生儿低血糖很常见,且可导致神经功能损害,但支持干预阈值的证据有限。
我们进行了一项前瞻性队列研究,纳入了528名胎龄至少35周且被认为有低血糖风险的新生儿;所有患儿均接受治疗以维持血糖浓度至少为每分升47毫克(每升2.6毫摩尔)。我们间歇性测量血糖长达7天。我们持续监测组织间液葡萄糖浓度,临床工作人员对其结果不知情。2岁时的评估包括贝利婴幼儿发育量表第三版以及执行功能和视觉功能测试。
在614名儿童中,528名符合条件,404名(占符合条件儿童的77%)接受了评估;216名儿童(53%)有新生儿低血糖(血糖浓度<每分升47毫克)。当治疗使血糖浓度维持在至少每分升47毫克时,低血糖与神经感觉损害这一主要结局的风险增加无关(风险比,0.95;95%置信区间[CI],0.75至1.20;P = 0.67),也与加工困难无关,加工困难定义为执行功能评分或运动连贯性阈值超过均值1.5个标准差(风险比,0.92;95%CI,0.56至1.51;P = 0.74)。在未被识别的低血糖患儿(仅组织间液葡萄糖浓度低)中,风险并未增加。最低血糖浓度、低血糖发作次数和事件以及负组织间液增量(组织间液葡萄糖浓度曲线上方且低于每分升47毫克的面积)也不能预测结局。
在这个队列中,当治疗使血糖浓度维持在至少每分升47毫克时,新生儿低血糖与不良神经结局无关。(由尤妮斯·肯尼迪·施赖弗国家儿童健康与人类发展研究所及其他机构资助。)