Wafula Sam W
Sexual and Reproductive Health Program, Population Council, Nairobi, Kenya.
BMC Womens Health. 2015 Oct 14;15:86. doi: 10.1186/s12905-015-0240-z.
Women are described as experiencing unmet need for contraception if they are fecund, sexually active and wish to postpone or limit childbearing but fail to use contraception to do so. The consequences of unmet need include unwanted pregnancy, induced abortions, school dropout due to pregnancy and premature maternal deaths. Global efforts aimed at addressing the adverse effects of unmet need abound. In Kenya, one in every four married women in the reproductive age bracket (15-49 years) has unmet need for contraception. Regional differences exist but the reasons behind these differences remain poorly understood. The purpose of this study was to examine the extent to which regional differentials in unmet need for contraception exists and to explain the regional differences in unmet need for contraception in Kenya.
The paper used the Kenya Demographic and Health Survey (2008/09) data. Unmet need for contraception was measured based on the revised estimates contained in the survey. Summary statistics were used to show the percentage differences in the values of selected covariates across the high and low unmet need zones. The dependent variable had three categories: no unmet need, unmet need for spacing and unmet need for limiting births. The categorical nature of this dependent variable which is not ordered in any way lends itself to the use of multinomial logistic regression. The paper applied the seemingly unrelated estimation (suest) test to ascertain whether the covariate coefficients between the high and low unmet need zones were different. Stata Version 13.0 was used for analysis.
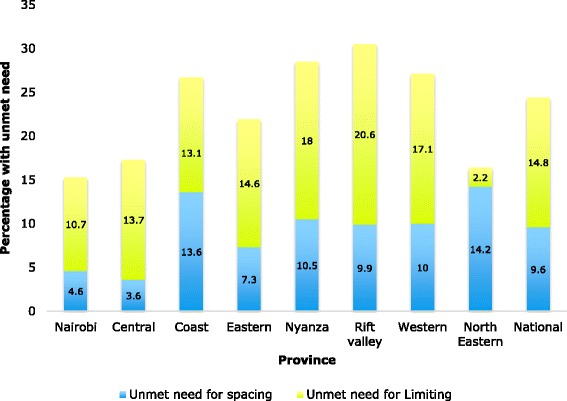
The percentage values of the selected covariates of unmet need for contraception were much higher in the high unmet need zone as compared to those observed in the low unmet need zones. On the overall, 15.4 % of women in the high unmet need zone had unmet need to space their next birth as compared to 8.6 % of their counterparts. Likewise, the percentage of women who wanted to limit further births stood at 14.1 % among women residing in high unmet need zones while those in low unmet need zones had 10.5 %. Further analysis based on seemingly unrelated estimation found that in general, a comparison of the coefficients been the high and low unmet need regions were significantly different (p < 0.05).
Evidence from the nationally representative KDHS 2008/09 shows that regional differentials in the covariates of unmet need for contraception exist. There is need to address religious inhibitions that stymie contraceptive uptake especially in the high unmet need regions. Efforts should promote maternal education and economically empower women in order to reinforce individual and contextual attitudes towards the benefits of contraception. The government should also establish social franchise programs to increase access to costly long acting and permanent methods of contraception to poor women.
如果育龄女性具有生育能力、有性行为且希望推迟或限制生育,但未采取避孕措施,那么就被视为有未满足的避孕需求。未满足避孕需求会带来诸多后果,包括意外怀孕、人工流产、因怀孕而辍学以及孕产妇过早死亡。全球为解决未满足避孕需求的不利影响做出了诸多努力。在肯尼亚,每四名处于生育年龄(15 - 49岁)的已婚女性中就有一人存在未满足的避孕需求。地区差异确实存在,但造成这些差异的原因仍知之甚少。本研究的目的是探究肯尼亚避孕需求未满足情况的地区差异程度,并解释这些地区差异背后的原因。
本文使用了肯尼亚人口与健康调查(2008/09)的数据。避孕需求未满足情况是根据该调查中的修订估计值来衡量的。描述性统计用于展示高避孕需求未满足地区和低避孕需求未满足地区选定协变量值的百分比差异。因变量有三个类别:无未满足需求、间隔生育的未满足需求以及限制生育的未满足需求。这个因变量的分类性质不存在任何顺序,适合使用多项逻辑回归。本文应用看似不相关估计(suest)检验来确定高避孕需求未满足地区和低避孕需求未满足地区的协变量系数是否不同。分析使用的是Stata 13.0版本。
与低避孕需求未满足地区相比,高避孕需求未满足地区选定的避孕需求未满足协变量的百分比值要高得多。总体而言,高避孕需求未满足地区15.4%的女性有间隔下一胎生育的未满足需求,而低避孕需求未满足地区这一比例为8.6%。同样,高避孕需求未满足地区希望限制进一步生育的女性比例为14.1%,而低避孕需求未满足地区为10.5%。基于看似不相关估计的进一步分析发现,总体而言,高避孕需求未满足地区和低避孕需求未满足地区的系数比较存在显著差异(p < 0.05)。
来自具有全国代表性的2008/09年肯尼亚人口与健康调查的证据表明,避孕需求未满足的协变量存在地区差异。有必要消除阻碍避孕措施采用的宗教禁忌,特别是在高避孕需求未满足地区。应努力促进孕产妇教育并增强妇女的经济权能,以强化个人和环境对避孕益处的态度。政府还应设立社会特许经营项目,以便贫困妇女能够更容易获得成本较高的长效和永久避孕方法。