Yaghi Shadi, Boehme Amelia K, Dibu Jamil, Leon Guerrero Christopher R, Ali Syed, Martin-Schild Sheryl, Sands Kara A, Noorian Ali Reza, Blum Christina A, Chaudhary Shuchi, Schwamm Lee H, Liebeskind David S, Marshall Randolph S, Willey Joshua Z
Department of Neurology, Columbia University Medical Center, New York, New York2currently with the Department of Neurology, Brown University, Providence, Rhode Island.
Department of Neurology, Columbia University Medical Center, New York, New York.
JAMA Neurol. 2015 Dec;72(12):1451-7. doi: 10.1001/jamaneurol.2015.2371.
Treatments for symptomatic intracerebral hemorrhage (sICH) are based on expert opinion, with limited data available on efficacy.
To better understand the natural history of thrombolysis-related sICH, with a focus on the efficacy of various treatments used.
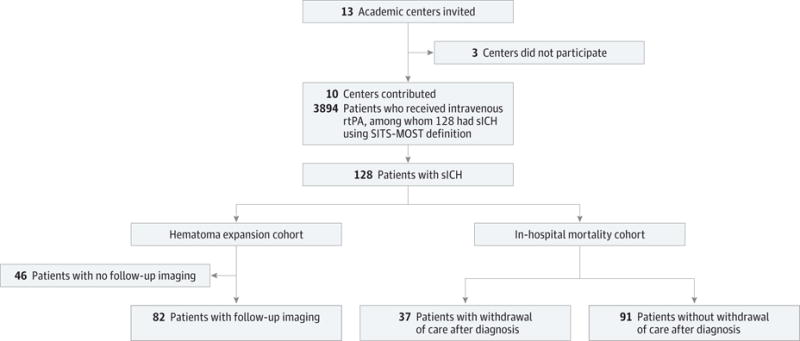
DESIGN, SETTING, AND PARTICIPANTS: Multicenter retrospective study between January 1, 2009, and April 30, 2014, at 10 primary and comprehensive stroke centers across the United States. Participants were all patients with sICH, using the definition by the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST), which included a parenchymal hematoma type 2 and at least a 4-point increase in the National Institutes of Health Stroke Scale score.
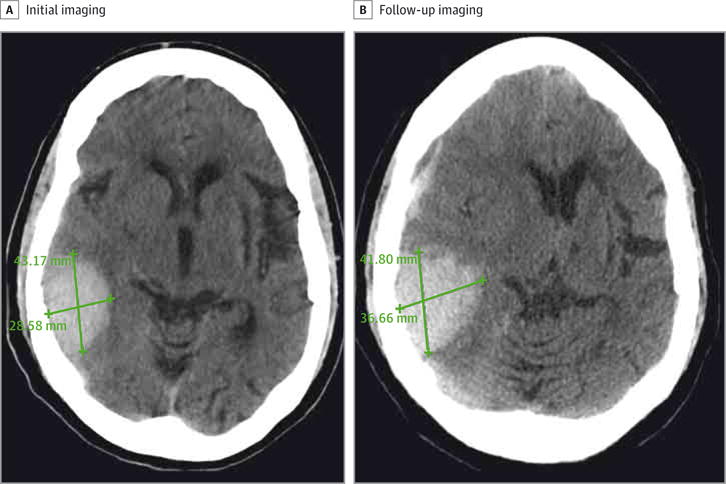
The primary outcome was in-hospital mortality, and the secondary outcome was hematoma expansion, defined as a 33% increase in the hematoma volume on follow-up imaging.
Of 3894 patients treated with intravenous recombinant tissue plasminogen activator (rtPA) within 4½ hours after symptom onset of ischemic stroke, 128 (3.3%) had sICH. The median time from initiation of rtPA therapy to sICH diagnosis was 470 minutes (range, 30-2572 minutes), and the median time from diagnosis to treatment of sICH was 112 minutes (range, 12-628 minutes). The in-hospital mortality rate was 52.3% (67 of 128), and 26.8% (22 of 82) had hematoma expansion. In the multivariable models, code status change to comfort measures after sICH diagnosis was the sole factor associated with increased in-hospital mortality (odds ratio, 3.6; 95% CI, 1.2-10.6). Severe hypofibrinogenemia (fibrinogen level, <150 mg/dL) was associated with hematoma expansion, occurring in 36.3% (8 of 22) of patients without hematoma expansion vs in 25.0% (15 of 60) of patients with hematoma expansion (P = .01), highlighting a role for cryoprecipitate in reversing rtPA coagulopathy.
In this study, treatment of postthrombolysis sICH did not significantly reduce the likelihood of in-hospital mortality or hematoma expansion. Shortening the time to diagnosis and treatment may be a key variable in improving outcomes of patients with sICH.
有症状性脑出血(sICH)的治疗基于专家意见,关于疗效的数据有限。
为了更好地了解溶栓相关sICH的自然病史,重点关注所使用的各种治疗方法的疗效。
设计、地点和参与者:2009年1月1日至2014年4月30日在美国10个初级和综合卒中中心进行的多中心回顾性研究。参与者为所有符合卒中溶栓安全实施监测研究(SITS-MOST)定义的sICH患者,该定义包括2型实质血肿且美国国立卫生研究院卒中量表评分至少增加4分。
主要结局是住院死亡率,次要结局是血肿扩大,定义为随访影像学上血肿体积增加33%。
在症状性缺血性卒中发病后4.5小时内接受静脉注射重组组织型纤溶酶原激活剂(rtPA)治疗的3894例患者中,128例(3.3%)发生了sICH。从开始rtPA治疗到sICH诊断的中位时间为470分钟(范围30 - 2572分钟),从sICH诊断到治疗的中位时间为112分钟(范围12 - 628分钟)。住院死亡率为52.3%(128例中的67例),26.8%(82例中的22例)发生了血肿扩大。在多变量模型中,sICH诊断后将医疗状态改为舒适护理措施是与住院死亡率增加相关的唯一因素(比值比,3.6;95%置信区间,1.2 - 10.6)。严重低纤维蛋白原血症(纤维蛋白原水平<150mg/dL)与血肿扩大相关,未发生血肿扩大的患者中有36.3%(22例中的8例)出现,而发生血肿扩大的患者中有25.0%(60例中的15例)出现(P = 0.01),这突出了冷沉淀在逆转rtPA凝血病中的作用。
在本研究中,溶栓后sICH的治疗并未显著降低住院死亡率或血肿扩大的可能性。缩短诊断和治疗时间可能是改善sICH患者结局的关键变量。