Bagaglio Sabrina, Uberti-Foppa Caterina, Di Serio Clelia, Trentini Filippo, Andolina Andrea, Hasson Hamid, Messina Emanuela, Merli Marco, Porrino Lucy, Lazzarin Adriano, Morsica Giulia
Infectious Diseases Department, Scientific Institute Ospedale San Raffaele, Via Stamira d'Ancona 20, 20127 Milan, Italy (SB, CU-F, AA, HH, EM, MM, AL, GM); Vita-Salute University Via Olgettina 58, 20132 Milan, Italy (SB, AL); University Centre for Statistics in the Biomedical Sciences (CUSSB) Vita-Salute San Raffaele University, Via Olgettina 58, 20132 Milan, Italy (CDS, FT); L. Bocconi University, Via R. Sarfatti 25, 20136 Milan, Italy (FT); Mol Med Spa, Via Olgettina 58, 20132 Milan, Italy (LP).
Medicine (Baltimore). 2015 Oct;94(43):e1876. doi: 10.1097/MD.0000000000001876.
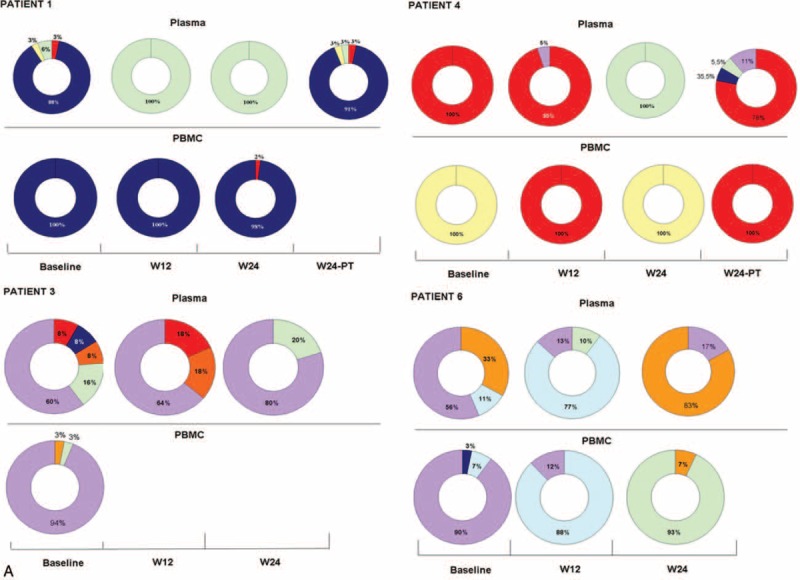
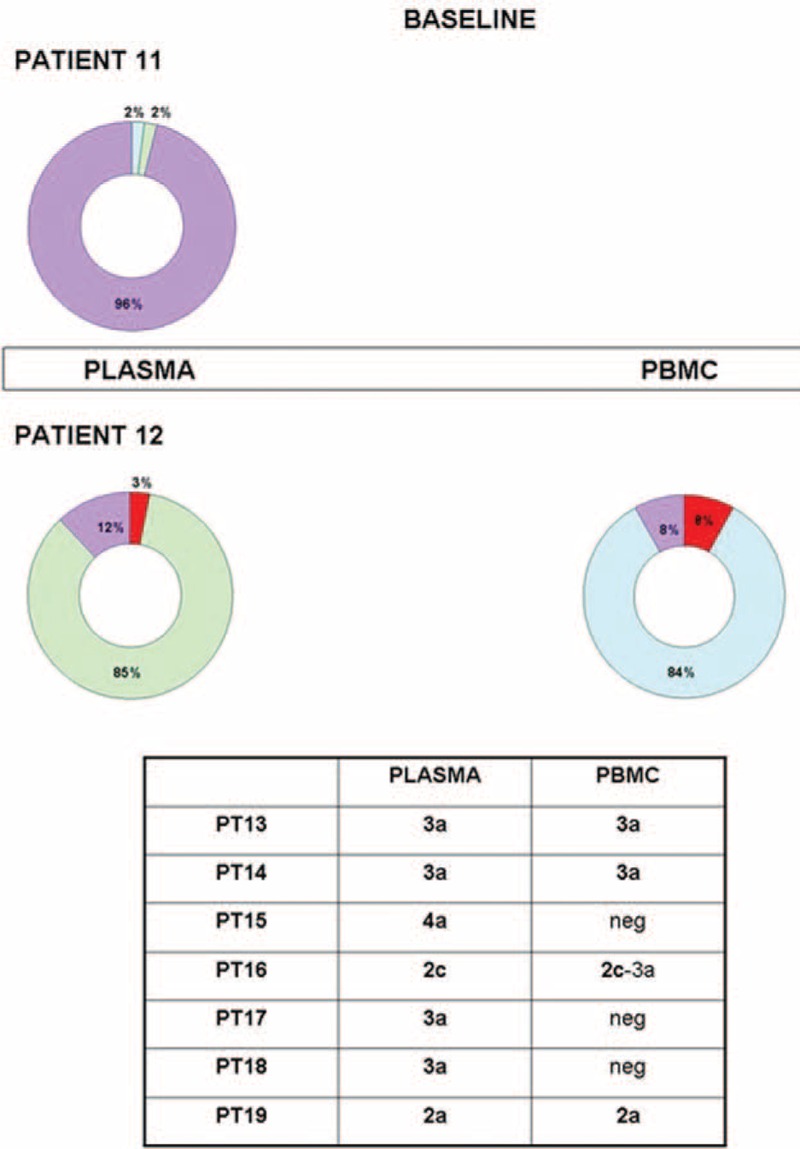
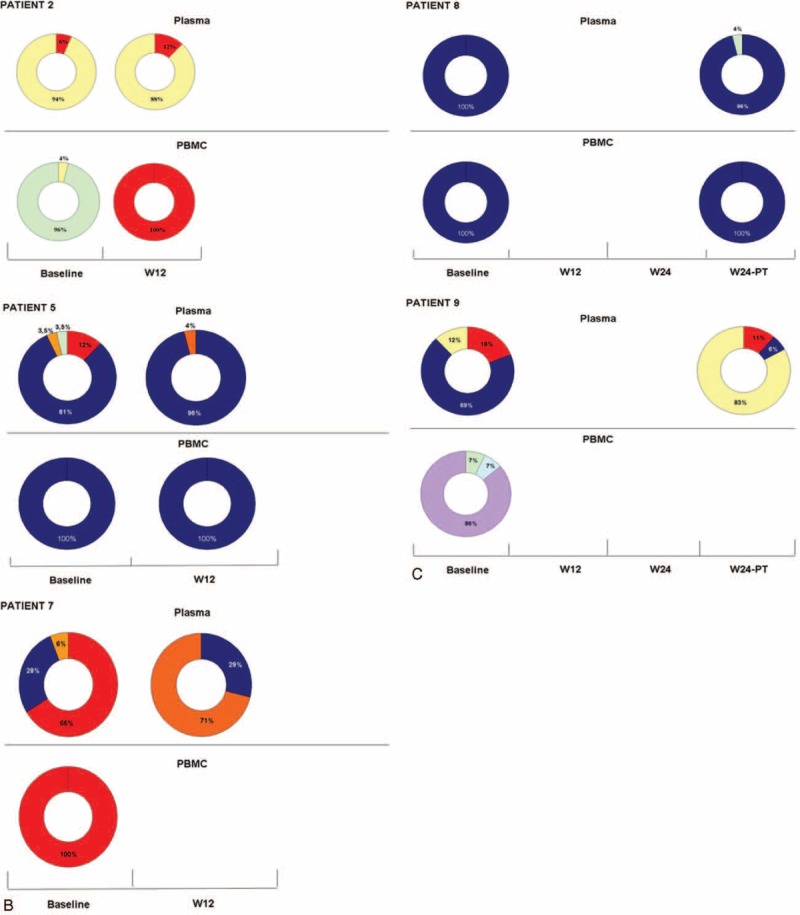
The extent of mixed hepatitis C virus (HCV) genotype in different compartments (plasma and peripheral blood mononuclear cell, PBMC) and possible association with treatment efficacy in HIV/HCV coinfected patients remains to be unknown.The objective of this study was to elucidate the frequency of mixed genotype infection (MG), its profile in different compartments during anti-HCV treatment, and the possible influence of different genotypes on the response rate.The compartmentalization of HCV population was investigated by next-generation sequencing in 19 HIV/HCV coinfected patients under anti-HCV treatment with peginterferon/ribavirin (P-R). Ten individuals were nonresponder (NR) or relapser (RE) to P-R treatment and 9 had a sustained virological response (SVR).Eleven/nineteen (58%) patients had MG in plasma compartment. Ten or 12 patients infected by a difficult to treat genotype (DTG) 1 or 4 as dominant strain, had an MG, whereas only 1/7 individuals infected by easy to treat genotype (ETG) harbored a mixed genotype, P = 0.006. HCV-RNA was more frequently detected in PBMC of NR (10/10) than in those of SVR (5/9), P = 0.032. Mixed genotype infection was detected in 6/15 (40%) PBMC-positive cases and was not associated with P-R treatment response. By multivariate analysis, MG in plasma samples was the most important viral factor affecting the treatment response (P = 0.0237).Detection of MG in plasma of HIV/HCV coinfected patients seems to represent the major determinant of response to P-R treatment. This finding may have important clinical implication in light of the new therapeutic approach in HIV/HCV coinfected individuals suggesting that combination treatment with direct acting antivirals could be less effective in MG.
在不同区室(血浆和外周血单个核细胞,PBMC)中丙型肝炎病毒(HCV)混合基因型的程度以及其与HIV/HCV合并感染患者治疗效果的可能关联仍不清楚。本研究的目的是阐明混合基因型感染(MG)的频率、抗HCV治疗期间其在不同区室中的特征以及不同基因型对缓解率的可能影响。通过下一代测序对19例接受聚乙二醇干扰素/利巴韦林(P-R)抗HCV治疗的HIV/HCV合并感染患者的HCV群体进行区室化研究。10例患者对P-R治疗无应答(NR)或复发(RE),9例有持续病毒学应答(SVR)。11/19(58%)的患者血浆区室存在MG。10或12例以难治性基因型(DTG)1或4为主导毒株感染的患者存在MG,而仅1/7例以易治性基因型(ETG)感染的个体携带混合基因型,P = 0.006。NR患者的PBMC中比SVR患者更频繁地检测到HCV-RNA(10/10比5/9),P = 0.032。在15例PBMC阳性病例中的6例(40%)检测到混合基因型感染,且与P-R治疗反应无关。通过多变量分析,血浆样本中的MG是影响治疗反应的最重要病毒因素(P = 0.0237)。在HIV/HCV合并感染患者血浆中检测到MG似乎是对P-R治疗反应的主要决定因素。鉴于HIV/HCV合并感染个体的新治疗方法,这一发现可能具有重要的临床意义,提示直接作用抗病毒药物联合治疗在MG患者中可能效果较差。