Wu Xiujuan, Zhang Bing, Li Chunrong, Shen Donghui, Liu Kangding, Zhu Jie, Zhang Hong-Liang
From the Neuroscience Center, Department of Neurology, the First Hospital of Jilin University, Jilin University, Changchun, China (XW, BZ, CL, DS, KL, JZ, H-LZ); and Department of Neurobiology, Care Sciences and Society, Karolinska Institute, Stockholm, Sweden (JZ).
Medicine (Baltimore). 2015 Oct;94(43):e1898. doi: 10.1097/MD.0000000000001898.
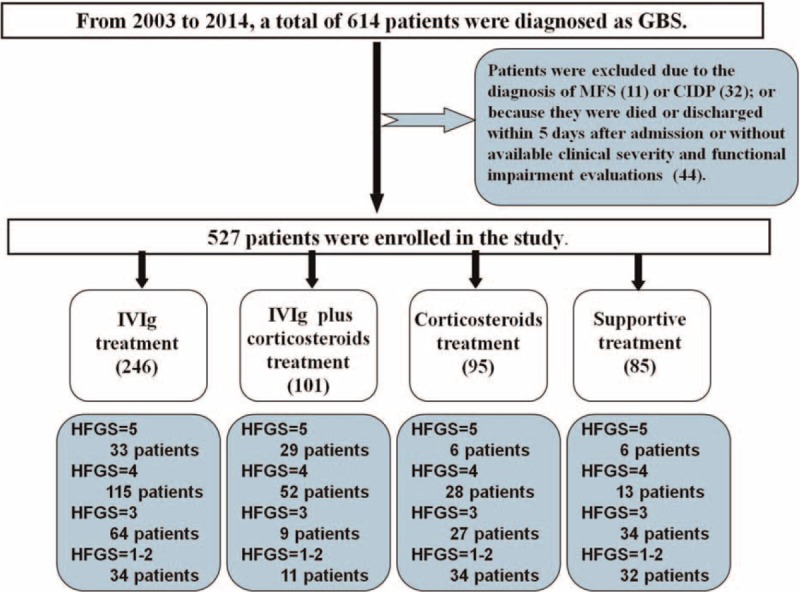
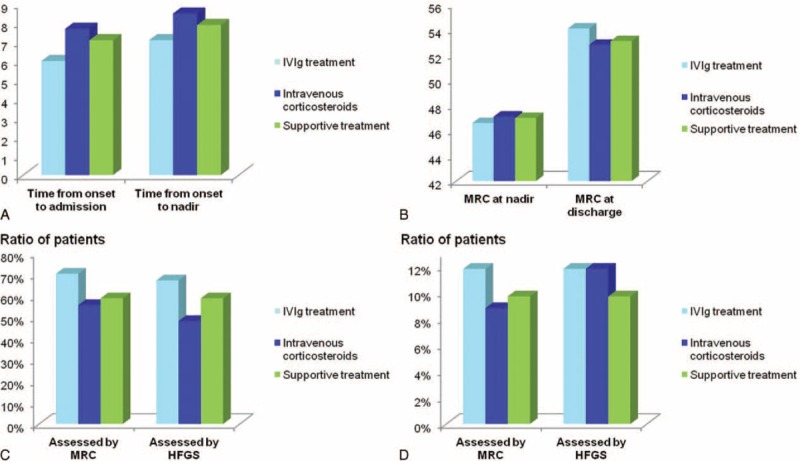
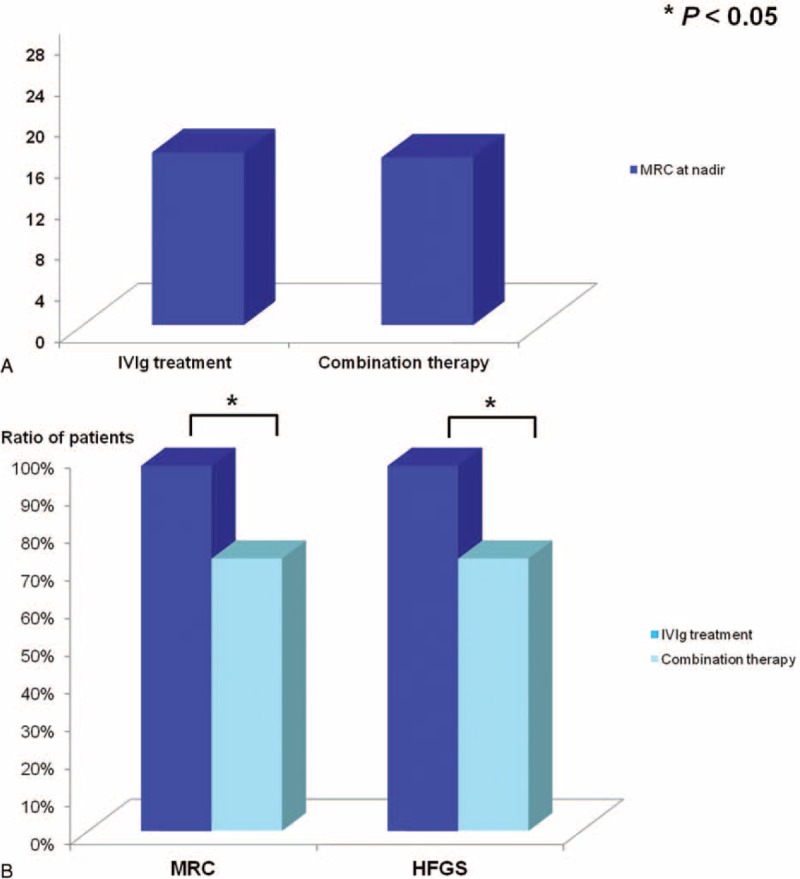
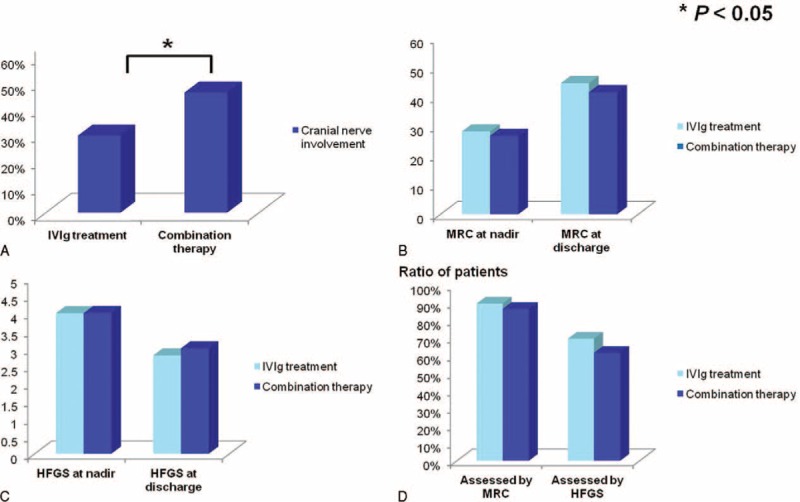
Intravenous immunoglobulin (IVIg) has been proven most effective in treating Guillain-Barré syndrome (GBS). Corticosteroids as an add-on therapy have been prescribed in severe GBS cases. However, the efficacy of intravenous corticosteroids combined with IVIg in dealing with severe GBS remains unclear. We explored the therapeutic effects of different therapeutic regimens on the short-term prognosis of GBS patients, especially the severe cases.We retrospectively analyzed the clinical data of 527 adult patients with GBS who were prescribed to different treatments from 2003 to 2014. The therapeutic effect of a treatment was evaluated by the improvement of Hughes Functional Grading Scale (HFGS) and Medical Research Council (MRC) sum score.With comparable incidence of infectious complications (P > 0.05), more mechanically ventilated patients were found improvement after IVIg treatment than combination IVIg with intravenous corticosteroids (MRC: 97% vs. 72.4%, P < 0.05; HFGS: 97% vs. 72.4%, P < 0.05). As to bedridden patients without mechanical ventilation, incidence of infectious complications (P > 0.05) and ratio of patients who were improved after IVIg were insignificantly different from the combination therapy (MRC: 89.6% vs. 86.5%; HFGS: 69.6% vs. 61.5%; both P > 0.05), even if the intravenous corticosteroids were initiated within 7 days after onset (P > 0.05). In addition, supportive treatment was sufficient for patients who were able to walk with help (HFGS = 3) and mildly affected (HFGS < 3) when compared with IVIg and intravenous corticosteroids.IVIg is sufficient to GBS patients who are unable to walk (HFGS > 3), while corticosteroids are detrimental for short-term prognosis in mechanically ventilated patients when used in combination with IVIg. Further prospective and randomized studies are warranted to validate this finding.
静脉注射免疫球蛋白(IVIg)已被证明在治疗吉兰-巴雷综合征(GBS)方面最为有效。在严重GBS病例中,已将皮质类固醇作为辅助治疗药物。然而,静脉注射皮质类固醇联合IVIg治疗严重GBS的疗效仍不明确。我们探讨了不同治疗方案对GBS患者,尤其是重症患者短期预后的治疗效果。我们回顾性分析了2003年至2014年期间接受不同治疗的527例成年GBS患者的临床资料。通过Hughes功能分级量表(HFGS)和医学研究委员会(MRC)总分的改善来评估治疗效果。在感染并发症发生率相当的情况下(P>0.05),发现接受IVIg治疗的机械通气患者改善情况比IVIg联合静脉注射皮质类固醇治疗的患者更多(MRC:97%对72.4%,P<0.05;HFGS:97%对72.4%,P<0.05)。对于无需机械通气的卧床患者,感染并发症发生率(P>0.05)以及IVIg治疗后改善的患者比例与联合治疗相比无显著差异(MRC:89.6%对86.5%;HFGS:69.6%对61.5%;均P>0.05),即使静脉注射皮质类固醇在发病后7天内开始使用(P>0.05)。此外,与IVIg和静脉注射皮质类固醇治疗相比,对于能够在帮助下行走(HFGS=3)和轻度受累(HFGS<~3)的患者,支持性治疗就足够了。对于无法行走的GBS患者(HFGS>3),IVIg治疗就足够了,而皮质类固醇与IVIg联合使用时对机械通气患者的短期预后有害。需要进一步进行前瞻性和随机研究来验证这一发现。