DeWitt John, Cho Chang-Min, Lin Jingmei, Al-Haddad Mohammad, Canto Marcia Irene, Salamone Ashley, Hruban Ralph H, Messallam Ahmed A, Khashab Mouen A
Department of Gastroenterology, Indiana University Health Medical Center, Indianapolis, Indiana, United States.
Department of Pathology, Indiana University Health Medical Center, Indianapolis, Indiana, United States.
Endosc Int Open. 2015 Oct;3(5):E471-8. doi: 10.1055/s-0034-1392222. Epub 2015 Jun 24.
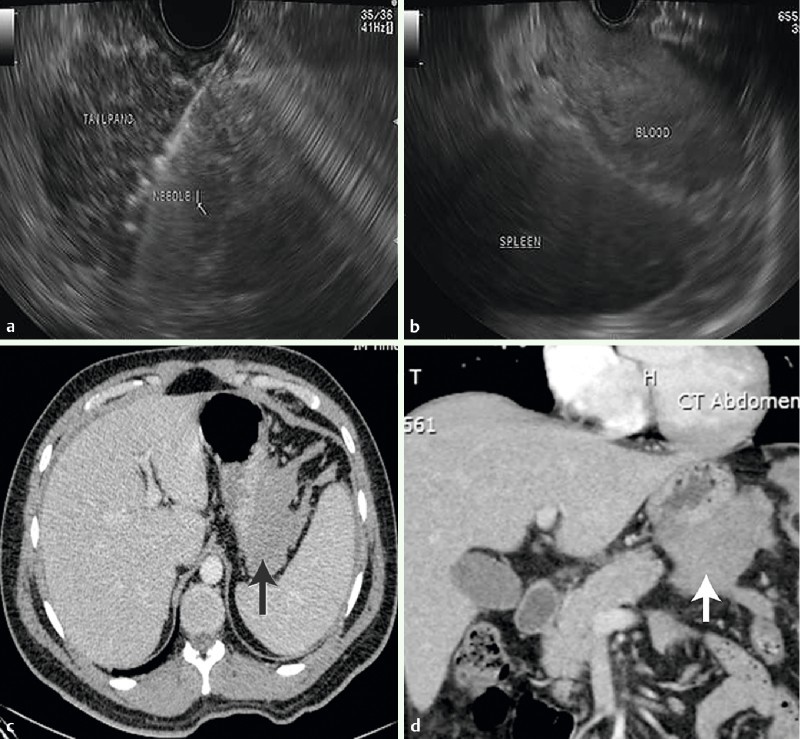
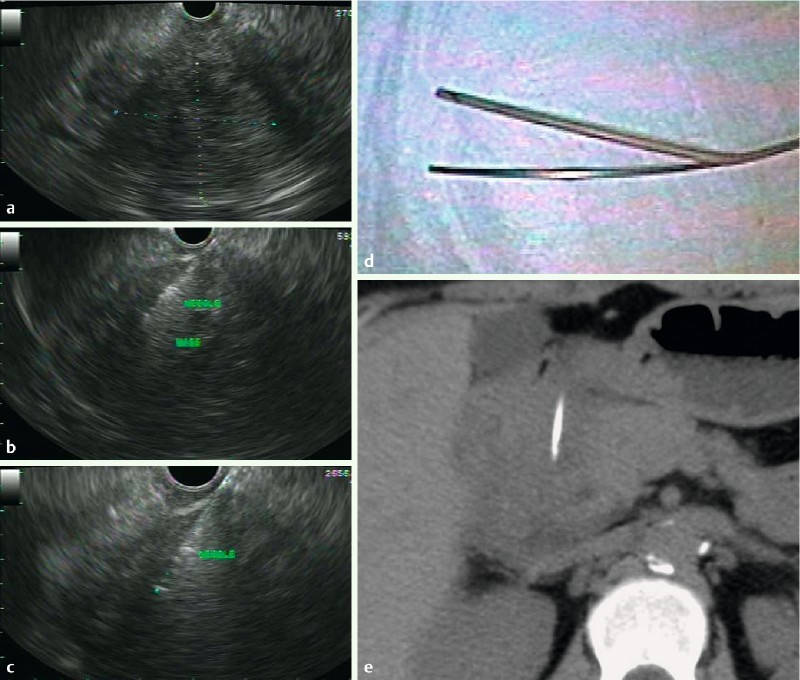
The optimal core biopsy needle for endoscopic ultrasound (EUS) is unknown. The principle aim of this study is to compare outcomes of EUS-fine-needle biopsy (EUS-FNB) with a new 19-gauge EUS histology needle (ProCore, Cook Medical Inc., Winston-Salem, North Carolina, United States) to a conventional 19-gauge Tru-Cut biopsy (EUS-TCB) needle (19G, Quick-Core, Cook Medical Inc.).
Patients referred for EUS who require possible histologic biopsy were prospectively randomized to EUS-FNB or EUS-TCB. With the initial needle, ≤ 3 biopsies were obtained until either technical failure or an adequate core was obtained. Patients with suspected inadequate biopsies were crossed over to the other needle and similarly ≤ 3 passes were obtained until adequate cores or technical failure occurred. Technical success, diagnostic histology, accuracy and complication rates were evaluated.
Eighty-five patients (mean 58 years; 43 male) were randomized to FNB (n = 44) and TCB (n = 41) with seven patients excluded. Procedure indication, biopsy site, mass size, number of passes, puncture site, overall technical success and adverse events were similar between the two groups. FNB specimens had a higher prevalence of diagnostic histology (85 % vs. 57 %; P = 0.006), accuracy (88 % vs. 62 %; P = 0.02), mean total length (19.4 vs. 4.3 mm; P = 0.001), mean complete portal triads from liver biopsies (10.4 vs. 1.3; P = 0.0004) and required fewer crossover biopsies compared to those of TCB (2 % vs. 65 %; P = 0.0001). Overall technical success and complication rates were comparable.
EUS-FNB using a 19-gauge FNB needle is superior to 19-gauge EUS-TCB needle.
目前尚不清楚用于内镜超声(EUS)的最佳活检针。本研究的主要目的是比较使用新型19G EUS组织学活检针(ProCore,库克医疗公司,美国北卡罗来纳州温斯顿 - 塞勒姆)进行内镜超声引导下细针穿刺活检(EUS - FNB)与传统19G Tru - Cut活检针(EUS - TCB,19G,Quick - Core,库克医疗公司)的效果。
对因EUS检查可能需要组织学活检的患者进行前瞻性随机分组,分为EUS - FNB组或EUS - TCB组。使用初始活检针,获取≤3次活检样本,直至出现技术失败或获得足够的组织芯。怀疑活检样本不足的患者改用另一活检针,同样获取≤3次穿刺样本,直至获得足够的组织芯或出现技术失败。评估技术成功率、诊断性组织学结果、准确性及并发症发生率。
85例患者(平均年龄58岁;男性43例)被随机分为FNB组(n = 44)和TCB组(n = 41),7例患者被排除。两组在手术指征、活检部位、肿块大小、穿刺次数、穿刺点、总体技术成功率及不良事件方面相似。FNB样本的诊断性组织学发生率更高(85%对57%;P = 0.006),准确性更高(88%对62%;P = 0.02),平均总长度更长(19.4对4.3 mm;P = 0.001),肝活检中平均完整门静脉三联征数量更多(10.4对1.3;P = 0.0004),与TCB相比需要的交叉活检更少(2%对65%;P = 0.0001)。总体技术成功率和并发症发生率相当。
使用19G FNB针进行EUS - FNB优于19G EUS - TCB针。