Toy Mehlika, Hutton David W, So Samuel K
Asian Liver Center, Department of Surgery, Stanford University School of Medicine, Stanford, CA, 94305, United States of America.
Department of Health Management and Policy, University of Michigan, Ann Arbor, MI, 48109, United States of America.
PLoS One. 2015 Nov 4;10(11):e0139876. doi: 10.1371/journal.pone.0139876. eCollection 2015.
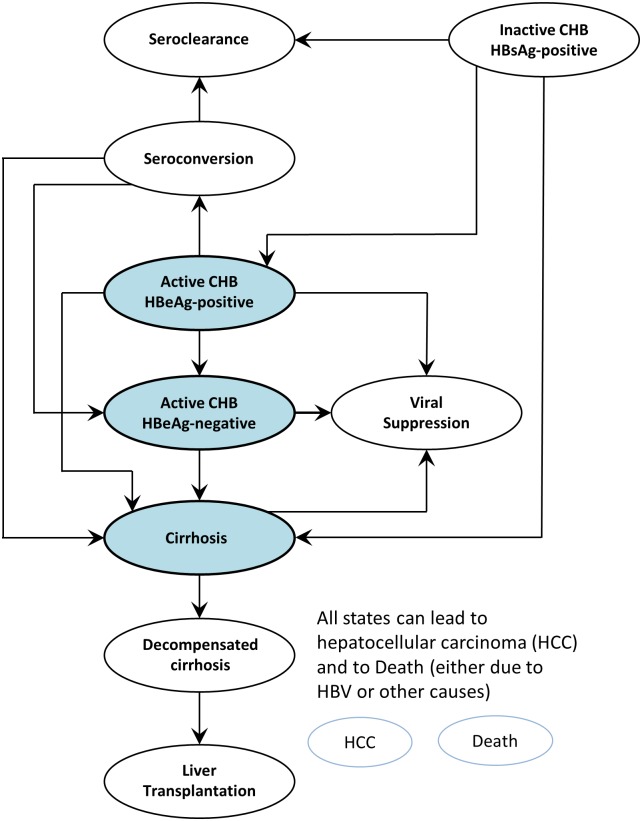
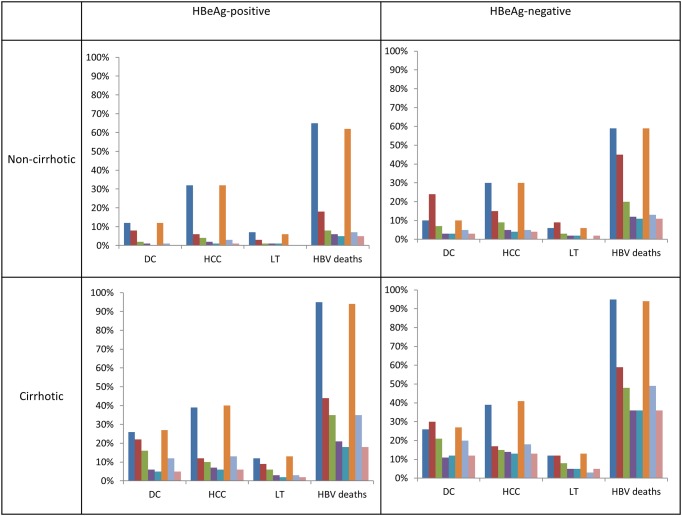
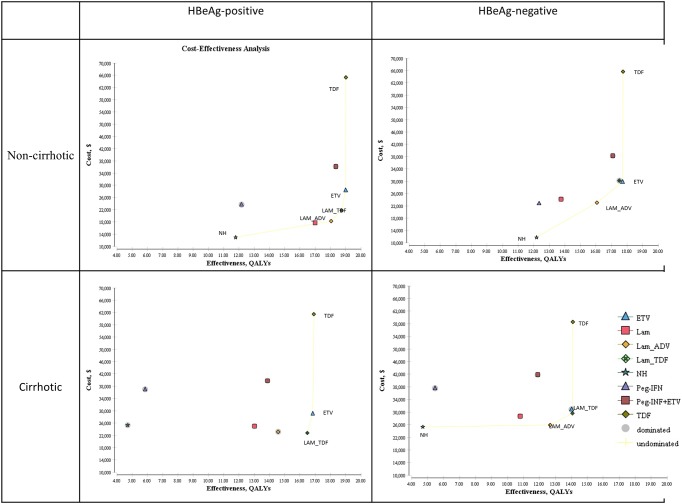
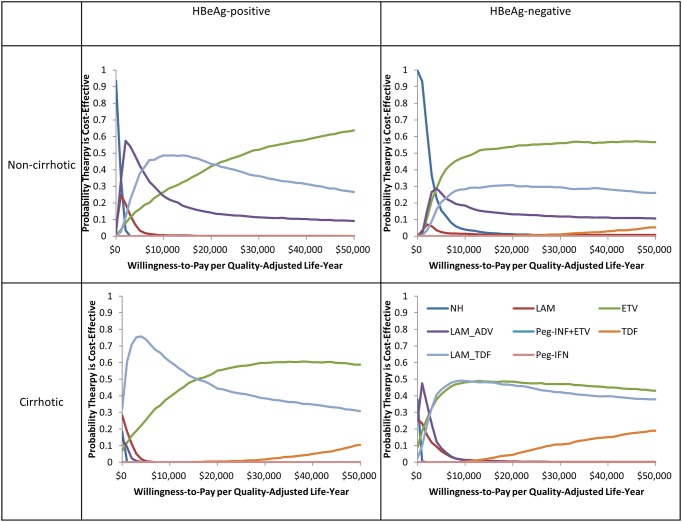
Chronic liver disease and liver cancer associated with chronic hepatitis B (CHB) are leading causes of death among adults in China. Although newborn hepatitis B immunization has successfully reduced the prevalence of CHB in children, about 100 million Chinese adults remain chronically infected. If left unmanaged, 15-25% will die from liver cancer or liver cirrhosis. Antiviral treatment is not necessary for all patients with CHB, but when it is indicated, good response to treatment would prevent disease progression and reduce disease mortality and morbidity, and costly complications. The aim of this study is to analyze the cost-effectiveness of generic and brand antiviral drugs for CHB treatment in China, and assessing various thresholds at which a highly potent, low resistance antiviral drug would be cost-saving and/or cost-effective to introduce in a national treatment program. We developed a Markov simulation model of disease progression using effectiveness and cost data from the medical literature. We measured life-time costs, quality adjusted life years (QALYs), incremental cost-effectiveness ratios (ICERs), and clinical outcomes. The no treatment strategy incurred the highest health care costs ($12,932-$25,293) per patient, and the worst health outcomes, compared to the antiviral treatment strategies. Monotherapy with either entecavir or tenofovir yielded the most QALYs (14.10-19.02) for both HBeAg-positive and negative patients, with or without cirrhosis. Threshold analysis showed entercavir or tenofovir treatment would be cost saving if the drug price is $32-75 (195-460 RMB) per month, highly cost-effective at $62-110 (379-670 RMB) per month and cost-effective at $63-120 (384-734 RMB) per month. This study can support policy decisions regarding the implementation of a national health program for chronic hepatitis B treatment in China at the population level.
慢性肝病和与慢性乙型肝炎(CHB)相关的肝癌是中国成年人死亡的主要原因。尽管新生儿乙肝疫苗接种已成功降低了儿童CHB的患病率,但仍有约1亿中国成年人处于慢性感染状态。如果不加以治疗,15%-25%的患者将死于肝癌或肝硬化。并非所有CHB患者都需要进行抗病毒治疗,但在有指征时,良好的治疗反应可预防疾病进展,降低疾病死亡率和发病率以及昂贵的并发症。本研究的目的是分析在中国使用仿制药和品牌抗病毒药物治疗CHB的成本效益,并评估在国家治疗计划中引入高效、低耐药抗病毒药物具有成本节约和/或成本效益的各种阈值。我们利用医学文献中的有效性和成本数据建立了疾病进展的马尔可夫模拟模型。我们测量了终身成本、质量调整生命年(QALY)、增量成本效益比(ICER)和临床结局。与抗病毒治疗策略相比,不治疗策略每位患者产生的医疗保健成本最高(12,932美元至25,293美元),健康结局最差。对于HBeAg阳性和阴性患者,无论有无肝硬化,恩替卡韦或替诺福韦单药治疗产生的QALY最多(14.10至19.02)。阈值分析表明,如果药物价格为每月32-75美元(195-460元人民币),恩替卡韦或替诺福韦治疗将具有成本节约效果;每月62-110美元(379-670元人民币)时具有高成本效益;每月63-120美元(384-734元人民币)时具有成本效益。本研究可为中国在人群层面实施慢性乙型肝炎国家治疗计划的政策决策提供支持。