Coles Alasdair
Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK.
Ann Indian Acad Neurol. 2015 Sep;18(Suppl 1):S30-4. doi: 10.4103/0972-2327.164824.
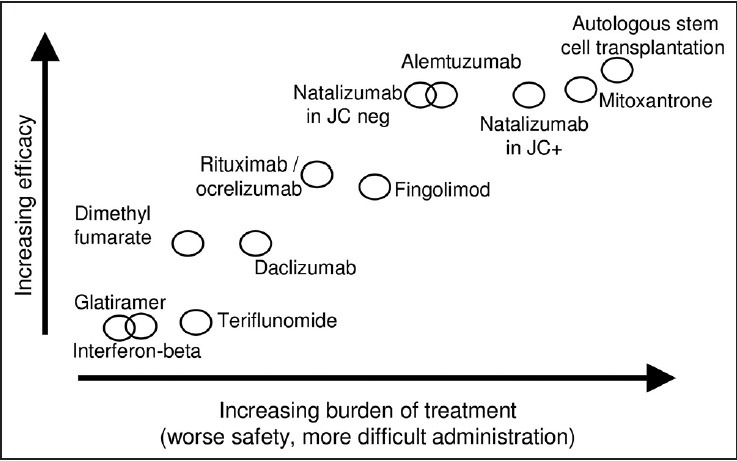
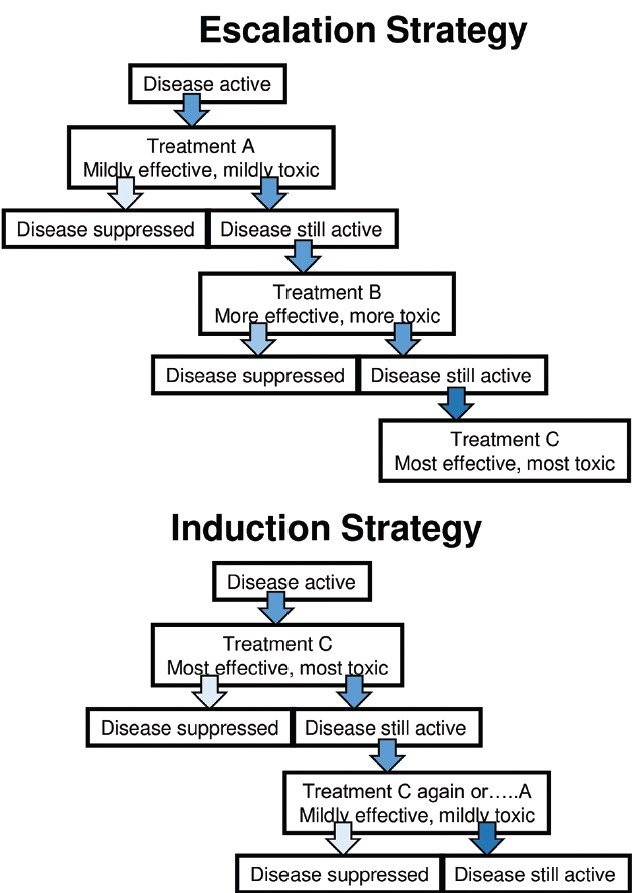
The newer immunotherapies for multiple sclerosis (fingolimod, natalizumab, dimethyl fumarate, teriflunomide, alemtuzumab) offer advantages of efficacy or tolerability over the injectable therapies of the 1990s. But they also have greater risks. As further treatments emerge (daclizumab and ocrelizumab are likely to be licensed in the next two years), the physician needs to be able to place them within a complex landscape of drugs and a specific treatment strategy, which may be an "escalation" or "induction" approach. Whilst on treatment, neurologist and patient need to be vigilant to signs of disease breakthrough or adverse effects.
用于治疗多发性硬化症的新型免疫疗法(芬戈莫德、那他珠单抗、富马酸二甲酯、特立氟胺、阿仑单抗)相较于20世纪90年代的注射疗法,在疗效或耐受性方面具有优势。但它们也有更大的风险。随着更多治疗方法的出现(达克珠单抗和奥瑞珠单抗可能在未来两年获批),医生需要能够将它们置于复杂的药物格局和特定的治疗策略中,这可能是一种“逐步升级”或“诱导”方法。在治疗期间,神经科医生和患者需要警惕疾病突破或不良反应的迹象。