Cecchini Reena S, Swain Sandra M, Costantino Joseph P, Rastogi Priya, Jeong Jong-Hyeon, Anderson Stewart J, Tang Gong, Geyer Charles E, Lembersky Barry C, Romond Edward H, Paterson Alexander H G, Wolmark Norman
NRG Oncology, Pittsburgh, Pennsylvania. University of Pittsburgh, Pittsburgh, Pennsylvania.
NRG Oncology/NSABP, Pittsburgh, Pennsylvania. Washington Cancer Institute, MedStar Washington Hospital Center, Washington, District of Columbia.
Cancer Epidemiol Biomarkers Prev. 2016 Jan;25(1):51-9. doi: 10.1158/1055-9965.EPI-15-0334-T. Epub 2015 Nov 6.
Body mass index (BMI) has been associated with breast cancer outcomes. However, few studies used clinical trial settings where treatments and outcomes are consistently evaluated and documented. There are also limited data assessing how patient/disease characteristics and treatment may alter the BMI-breast cancer association.
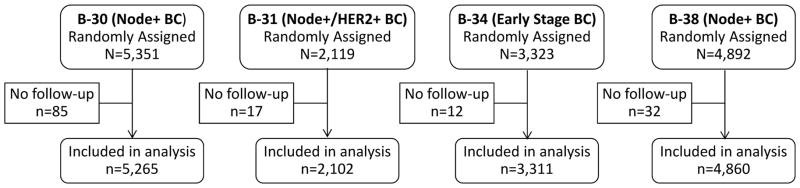
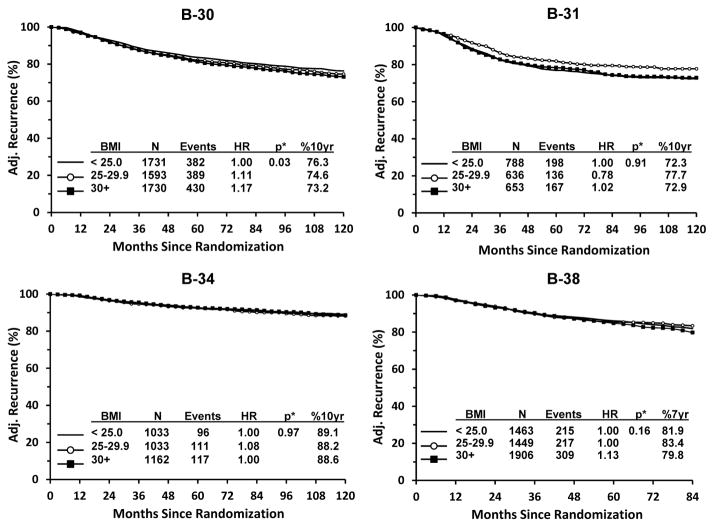
We evaluated 15,538 breast cancer participants from four NSABP protocols. B-34 studied early-stage breast cancer patients (N = 3,311); B-30 and B-38 included node-positive breast cancer patients (N = 5,265 and 4,860); and B-31 studied node-positive and HER2-positive breast cancer patients (N = 2,102). We used Cox proportional hazards regression to calculate adjusted hazards ratios (HR) for risk of death and recurrence, and conducted separate analyses by estrogen receptor (ER) status and treatment group.
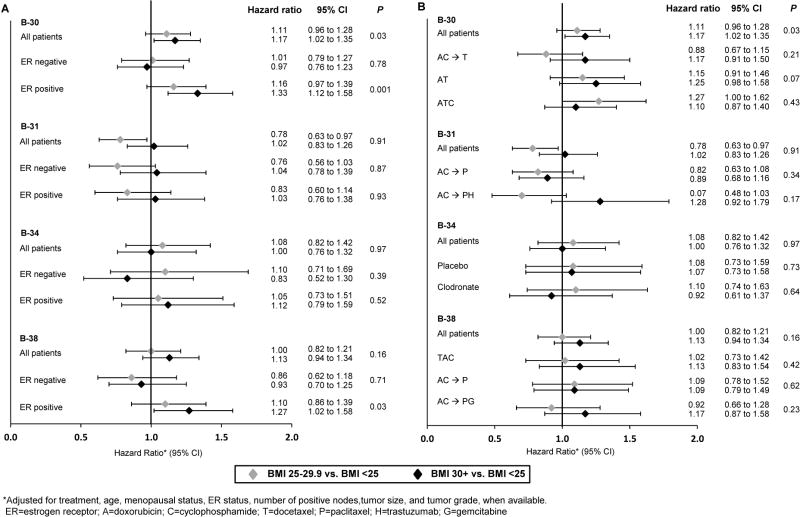
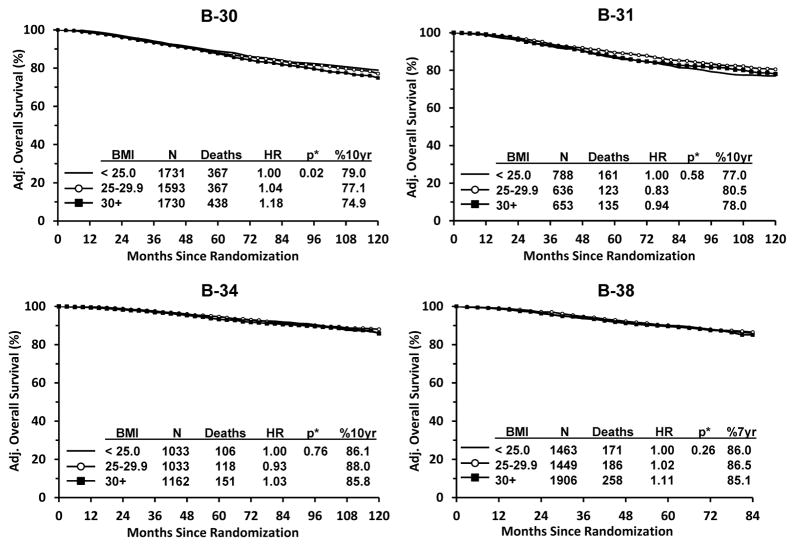
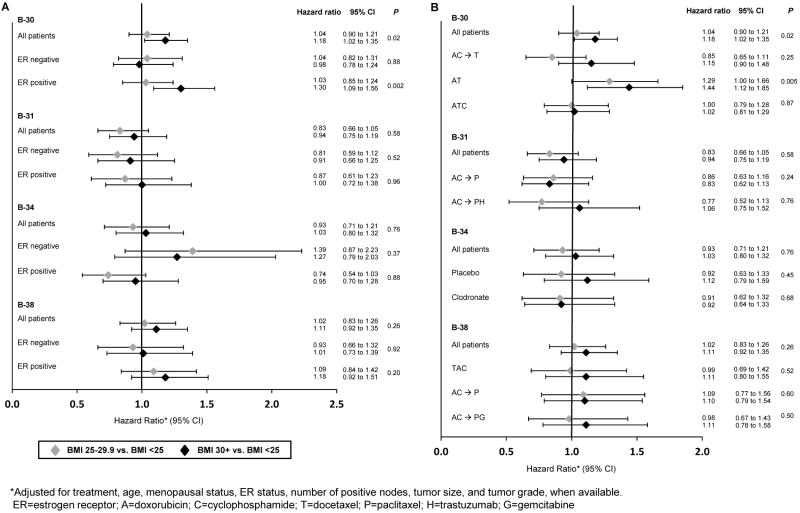
In B-30, increased BMI was significantly related to survival. Compared with BMI < 25, HRs were 1.04 for BMI 25 to 29.9 and 1.18 for BMI ≥ 30 (P = 0.02). Separate analyses indicated the significant relationship was only in ER-positive disease (P = 0.002) and the subgroup treated with doxorubicin/cyclophosphamide (P = 0.005). There were no significant trends across BMI for the other three trials. Similar results were found for recurrence. Increased BMI was significantly related to recurrence in B-30 (P = 0.03); and the significant relationship was only in ER-positive breast cancers (P = 0.001). Recurrence was also significant among ER-positive disease in B-38 (P = 0.03).
In our investigation, we did not find a consistent relationship between BMI at diagnosis and breast cancer recurrence or death.
This work demonstrates that the heterogeneity of breast cancer between different breast cancer populations and the different therapies used to treat them may modify any association that exists between BMI and breast cancer outcome.
体重指数(BMI)与乳腺癌预后相关。然而,很少有研究采用临床试验环境,在这种环境中对治疗方法和预后进行持续评估和记录。评估患者/疾病特征及治疗如何改变BMI与乳腺癌关联的数据也很有限。
我们评估了来自四项NSABP方案的15538名乳腺癌参与者。B-34研究早期乳腺癌患者(N = 3311);B-30和B-38纳入了淋巴结阳性乳腺癌患者(N = 5265和4860);B-31研究淋巴结阳性且人表皮生长因子受体2(HER2)阳性乳腺癌患者(N = 2102)。我们使用Cox比例风险回归来计算死亡和复发风险的调整风险比(HR),并按雌激素受体(ER)状态和治疗组进行单独分析。
在B-30中,BMI升高与生存显著相关。与BMI < 25相比,BMI为25至29.9时HR为1.04,BMI≥30时HR为1.18(P = 0.02)。单独分析表明,显著关系仅存在于ER阳性疾病(P = 0.002)和接受多柔比星/环磷酰胺治疗的亚组中(P = 0.005)。其他三项试验中,BMI并无显著趋势。复发情况也有类似结果。BMI升高与B-30中的复发显著相关(P = 0.03);且显著关系仅存在于ER阳性乳腺癌中(P = 0.001)。B-38中ER阳性疾病的复发也具有显著性(P = 0.03)。
在我们的研究中,我们未发现诊断时的BMI与乳腺癌复发或死亡之间存在一致关系。
这项研究表明,不同乳腺癌人群之间乳腺癌的异质性以及用于治疗它们的不同疗法可能会改变BMI与乳腺癌预后之间存在的任何关联。