Garner Alan A, Barker Claire L, Weatherall Andrew D
CareFlight, 4 Barden Street, Northmead, NSW 2152, Sydney, Australia.
Scand J Trauma Resusc Emerg Med. 2015 Nov 6;23:92. doi: 10.1186/s13049-015-0177-0.
Drowning patients may benefit from the advanced airway management capabilities that can be provided by physician staffed helicopter emergency medical services. The aim of this study is to describe paediatric drowning patients treated by such a service examining tasking systems, initial physiology at the incident scene, survival and neurological outcome.
Retrospective analysis of paediatric drowning victims over a 5- year period. Case identification system, patient age, site of drowning, presence or absence of cardiac output, first Glasgow Coma Scale (GCS) score and interventions were collected from prehospital notes, and survival and neurological outcomes from hospital and rehabilitation notes.
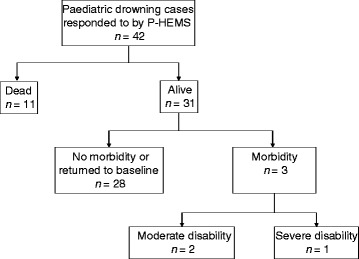
The P-HEMS direct case identification system operating in parallel with a central control system identified all severe drowning cases but 3 of 7 cases (43%) were missed when the central control system operated in isolation. All severe drowning cases (22) identified for P-HEMS response were intubated and transported directly to a paediatric specialist centre. Intubation required adjuvant anaesthesia in 10 (45%) cases. All children with GCS greater than eight on arrival of the P-HEMS survived neurologically intact. Seven of eight children with a GCS between four and seven survived without neurological impairment and all children with a GCS greater than three survived. Four of twelve asystolic children survived including one child who at 18 months post drowning is neurologically normal. All children who survived had return of spontaneous circulation prior to arrival in the emergency department.
P-HEMS played a significant role in the management of severe paediatric drowning in this case series. Requirement for P-HEMS only interventions were high and all identified cases were transferred directly to a paediatric specialist centre. Discontinuation of the P-HEMS direct case identication system that operated during the majority of the study period resulted in deterioration in system performance with some paediatric drowning cases subsequently not identified for P-HEMS response being transported to adult hospitals.
溺水患者可能会从由医生配备的直升机紧急医疗服务所提供的高级气道管理能力中获益。本研究的目的是描述接受此类服务治疗的小儿溺水患者,检查任务分配系统、事件现场的初始生理状况、生存率和神经学转归。
对5年期间的小儿溺水受害者进行回顾性分析。从院前记录中收集病例识别系统、患者年龄、溺水地点、有无心输出量、首次格拉斯哥昏迷量表(GCS)评分及干预措施,并从医院和康复记录中收集生存率和神经学转归情况。
与中央控制系统并行运行的P-HEMS直接病例识别系统识别出了所有严重溺水病例,但当中央控制系统单独运行时,7例中有3例(43%)被漏诊。确定由P-HEMS响应的所有严重溺水病例(22例)均进行了气管插管并直接转运至儿科专科中心。10例(45%)病例插管时需要辅助麻醉。P-HEMS到达时GCS大于8分的所有儿童神经功能均完好存活。8例GCS在4至7分之间的儿童中有7例存活且无神经功能损害,所有GCS大于3分的儿童均存活。12例心搏停止的儿童中有4例存活,其中1例溺水后18个月神经功能正常。所有存活的儿童在到达急诊科之前均恢复了自主循环。
在本病例系列中,P-HEMS在严重小儿溺水的管理中发挥了重要作用。仅需P-HEMS干预的比例很高且所有识别出的病例均直接转运至儿科专科中心。在研究的大部分时间里运行的P-HEMS直接病例识别系统停用后,系统性能恶化,一些未被识别为P-HEMS响应的小儿溺水病例随后被转运至成人医院。