Knarborg Malene, Hilberg Ole, Hoffmann Hans-Jürgen, Dahl Ronald
Department of Pulmonary Medicine and Allergology, Aarhus University Hospital, Aarhus, Denmark.
Department of Pulmonary Medicine and Allergology, Aarhus University Hospital, Aarhus, Denmark ; Department of Clinical Medicine, Aarhus University Hospital, Aarhus, Denmark.
Eur Clin Respir J. 2014 Nov 14;1. doi: 10.3402/ecrj.v1.25037. eCollection 2014.
Sustained use of oral corticosteroids is associated with significant side effects. It is therefore of interest to find a corticosteroid-sparing agent. In two meta-analyses, methotrexate resulted in a rather small reduction in the oral corticosteroid maintenance dose. We have used methotrexate as an oral corticosteroid-sparing agent in consecutive patients with severe bronchial asthma and find a need for a real-life observational study to evaluate the effect of methotrexate in clinical practice.
We analyzed the clinical data of 13 oral corticosteroid-dependent asthma patients with a mean prednisolone dose of 15 mg/day for up to 8 years. The diagnosis of asthma based on the clinical history, positive bronchodilator reversibility test, and variable airflow obstruction was secured by bronchial biopsies in all patients. We reviewed the literature and found 12 studies evaluating methotrexate as an oral corticosteroid-sparing agent in severe asthma and calculated the mean daily reduction in mg of prednisolone.
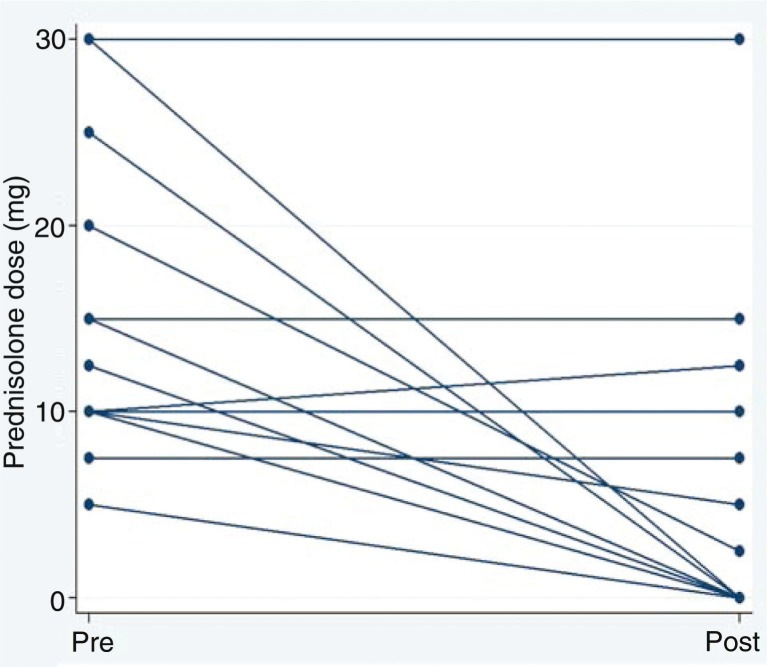
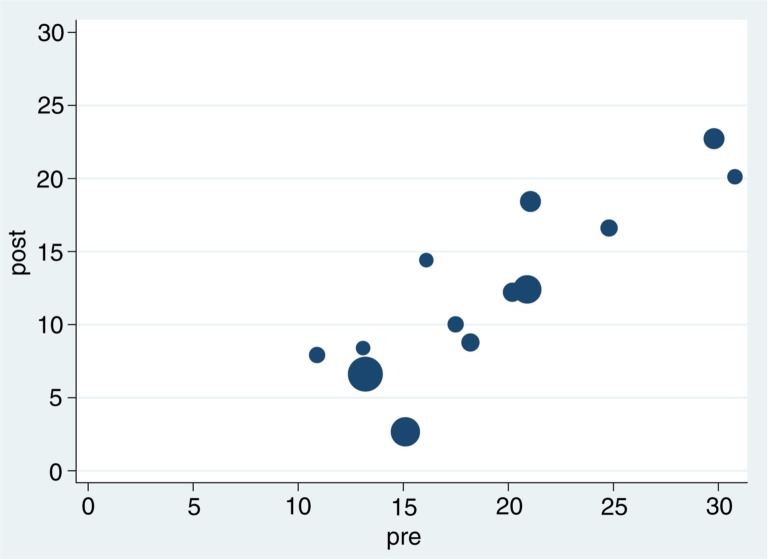
Oral corticosteroids could be reduced in 8/13 patients, 61.5% (mean reduction 9.0 mg/day), and stopped in six of these patients. Five patients had no reduction and remained oral corticosteroid-dependent. Patients with the highest oral corticosteroid doses experienced the greatest reductions. Two patients stopped methotrexate due to side effects. FEV1 remained unaffected by methotrexate treatment and corticosteroid reduction.
Methotrexate has significant oral corticosteroid-sparing effect while maintaining an unaltered asthma control and spirometry. Methotrexate seems an effective oral corticosteroid-sparing agent in a significant proportion of patients with severe asthma. The specific asthma phenotype/endotype that responds needs further study.
长期使用口服糖皮质激素会带来显著的副作用。因此,寻找一种能减少糖皮质激素用量的药物很有意义。在两项荟萃分析中,甲氨蝶呤使口服糖皮质激素维持剂量有较小幅度的降低。我们在连续的重度支气管哮喘患者中使用甲氨蝶呤作为口服糖皮质激素减量药物,并发现需要进行一项实际观察性研究来评估甲氨蝶呤在临床实践中的效果。
我们分析了13例依赖口服糖皮质激素的哮喘患者的临床资料,这些患者平均泼尼松龙剂量为15毫克/天,观察时间长达8年。所有患者均根据临床病史、支气管扩张剂可逆性试验阳性以及气流受限情况诊断为哮喘,并通过支气管活检确诊。我们查阅文献,发现12项评估甲氨蝶呤作为重度哮喘口服糖皮质激素减量药物的研究,并计算了泼尼松龙每日平均减少的毫克数。
13例患者中有8例(61.5%)口服糖皮质激素用量减少(平均减少9.0毫克/天),其中6例停用。5例患者用量未减少,仍依赖口服糖皮质激素。口服糖皮质激素剂量最高的患者减量幅度最大。2例患者因副作用停用甲氨蝶呤。甲氨蝶呤治疗及糖皮质激素减量对第一秒用力呼气容积(FEV1)无影响。
甲氨蝶呤在维持哮喘控制和肺功能测定不变的情况下,具有显著的减少口服糖皮质激素用量的作用。在相当一部分重度哮喘患者中,甲氨蝶呤似乎是一种有效的口服糖皮质激素减量药物。对甲氨蝶呤有反应的特定哮喘表型/内型需要进一步研究。