Maugeri Rosario, Anderson David Greg, Graziano Francesca, Meccio Flavia, Visocchi Massimiliano, Iacopino Domenico Gerardo
Department of Experimental Biomedicine and Clinical Neurosciences, School of Medicine, Neurosurgical Clinic, University of Palermo, Palermo, Italy.
Department of Orthopaedic, Surgery Rothman Institute, Philadelphia, PA, USA.
Am J Case Rep. 2015 Nov 14;16:811-7. doi: 10.12659/ajcr.895231.
Trauma is the leading cause of death in people younger than 45 years and head injury is the main cause of trauma mortality. Although epidural hematomas are relatively uncommon (less than 1% of all patients with head injuries and fewer than 10% of those who are comatose), they should always be considered in evaluation of a serious head injury. Patients with epidural hematomas who meet surgical criteria and receive prompt surgical intervention can have an excellent prognosis, presumably owing to limited underlying primary brain damage from the traumatic event. The decision to perform a surgery in a patient with a traumatic extraaxial hematoma is dependent on several factors (neurological status, size of hematoma, age of patients, CT findings) but also may depend on the judgement of the treating neurosurgeon.
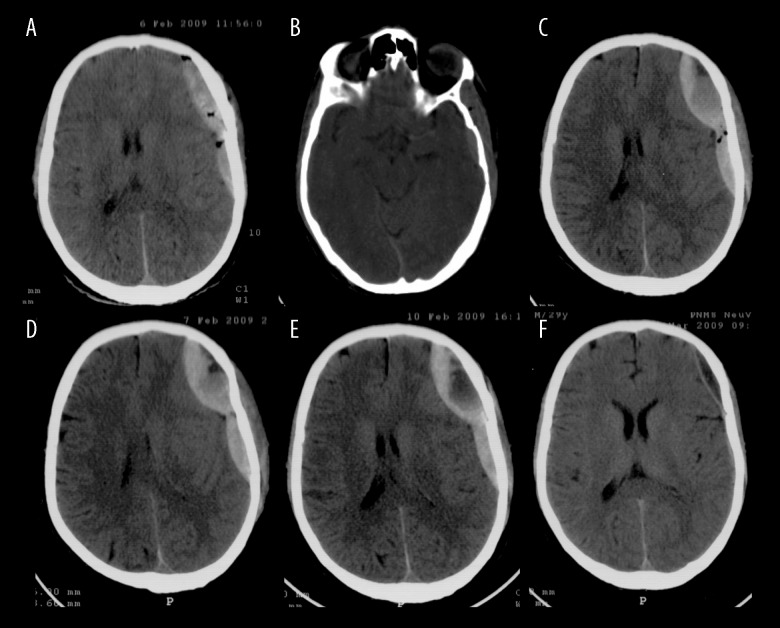
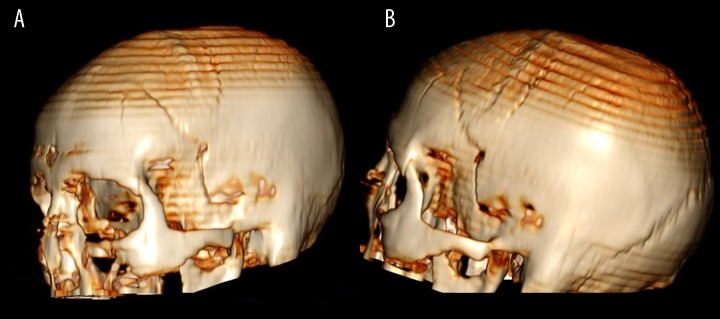
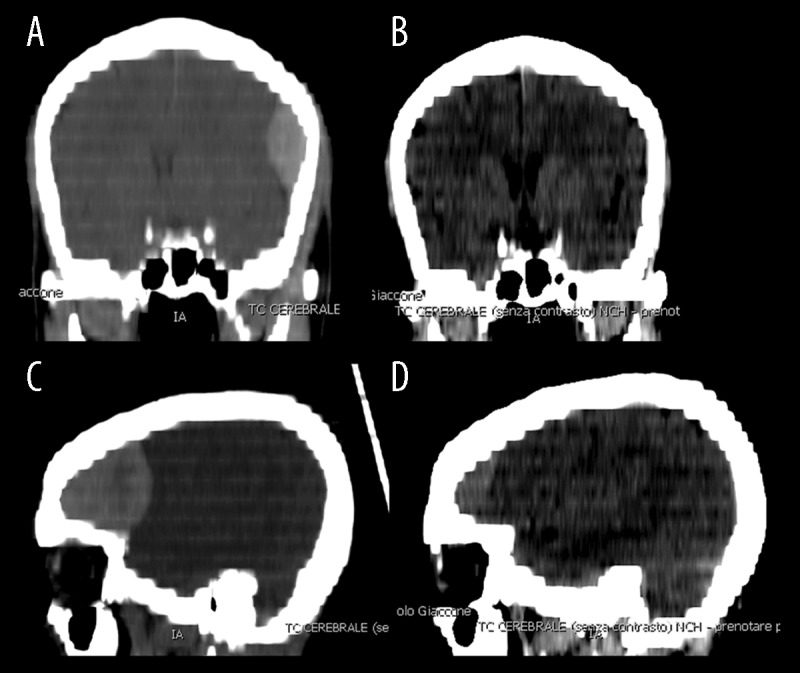
A 30-year old man arrived at our Emergency Department after a traumatic brain injury. General examination revealed severe headache, no motor or sensory disturbances, and no clinical signs of intracranial hypertension. A CT scan documented a significant left fronto-parietal epidural hematoma, which was considered suitable for surgical evacuation. The patient refused surgery. Following CT scan revealed a minimal increase in the size of the hematoma and of midline shift. The neurologic examination maintained stable and the patient continued to refuse the surgical treatment. Next follow up CT scans demonstrated a progressive resorption of hematoma.
We report an unusual case of a remarkable epidural hematoma managed conservatively with a favorable clinical outcome. This case report is intended to rather add to the growing knowledge regarding the best management for this serious and acute pathology.
创伤是45岁以下人群的主要死因,而头部损伤是创伤致死的主要原因。尽管硬膜外血肿相对少见(在所有头部损伤患者中占比不到1%,在昏迷患者中占比不到10%),但在评估严重头部损伤时应始终予以考虑。符合手术标准并接受及时手术干预的硬膜外血肿患者预后良好,这可能是由于创伤事件导致的潜在原发性脑损伤有限。对于创伤性轴外血肿患者,是否进行手术取决于多种因素(神经状态、血肿大小、患者年龄、CT表现),但也可能取决于主治神经外科医生的判断。
一名30岁男性在颅脑损伤后抵达我院急诊科。全身检查显示严重头痛,无运动或感觉障碍,无颅内高压的临床体征。CT扫描显示左侧额顶叶有明显的硬膜外血肿,被认为适合手术清除。患者拒绝手术。后续CT扫描显示血肿大小及中线移位略有增加。神经检查保持稳定,患者继续拒绝手术治疗。接下来的随访CT扫描显示血肿逐渐吸收。
我们报告了一例罕见的硬膜外血肿病例,采用保守治疗取得了良好的临床效果。本病例报告旨在增加对这种严重急性疾病最佳治疗方法的认识。