Zhao Li, Sun Tao, Sun Bao-Zhi, Zhao Yu-Hong, Norcini John, Chen Lincoln
School of Public Health, Harbin Medical University, Harbin, China.
Beijing Tian Tan Hospital, Capital Medical University, Beijing, China.
BMC Med Educ. 2015 Nov 25;15:207. doi: 10.1186/s12909-015-0495-y.
China adopted a Flexnerian model as its medical institutions developed over the recent past but the political, social, and economic environment has changed significantly since then. This has generated the need for educational reform, which in other countries, has largely been driven by competencies-oriented models such as those developed in Canada, and the United States. Our study sought to establish the competencies model, relevant to China, which will support educational reform efforts.
Data was collected using a cross-sectional survey of 1776 doctors from seven provinces in China. The surveys were translated and adapted from the Occupational Information Network General Work Activity questionnaire (ONET-GWA) and Work Style questionnaire (ONET-WS) developed under the auspices of the US Department of Labor. Exploratory factor analysis and confirmatory factor analysis ascertained the latent dimensions of the questionnaires, as well as the factor structures of the competencies model for the Chinese doctors.
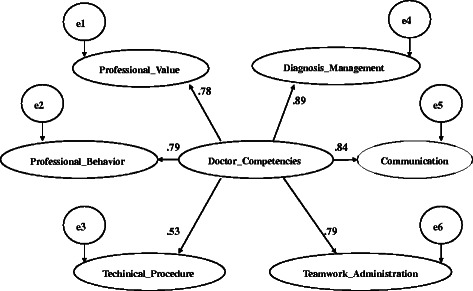
In exploratory factor analysis, the questionnaires were able to account for 64.25 % of total variance. All responses had high internal consistency and reliability. In confirmatory factor analysis, the loadings of six constructs were between 0.53 ~ 0.89 and were significant, Construct reliability (CR) were between 0.79 ~ 0.93 respectively. The results showed good convergent validity. The resultant models fit the data well (GFI was 0.92, RMSEA was 0.07) and the six-factor competencies framework for Chinese doctors emerged.
The Chinese doctors' competencies framework includes six elements: (a) technical procedural skills; (b) diagnosis and management; (c) teamwork and administration; (d) communication; (e) professional behavior; and (f) professional values. These findings are relevant to China, consistent with its current situation, and similar to those developed in other countries.
在过去一段时间里,随着中国医疗机构的发展,采用了弗莱克斯纳模式,但自那时以来,政治、社会和经济环境发生了重大变化。这就产生了教育改革的需求,在其他国家,这种改革很大程度上是由以能力为导向的模式推动的,比如加拿大和美国所开发的模式。我们的研究旨在建立与中国相关的能力模式,以支持教育改革努力。
通过对来自中国七个省份的1776名医生进行横断面调查来收集数据。这些调查问卷是根据美国劳工部主持开发的职业信息网络通用工作活动问卷(ONET-GWA)和工作方式问卷(ONET-WS)翻译和改编而来的。探索性因素分析和验证性因素分析确定了问卷的潜在维度,以及中国医生能力模式的因素结构。
在探索性因素分析中,问卷能够解释总方差的64.25%。所有回答都具有较高的内部一致性和可靠性。在验证性因素分析中,六个构念的载荷在0.53至0.89之间且具有显著性,构念可靠性(CR)分别在0.79至0.93之间。结果显示出良好的收敛效度。所得模型与数据拟合良好(GFI为0.92,RMSEA为0.07),中国医生的六因素能力框架得以呈现。
中国医生的能力框架包括六个要素:(a)技术程序技能;(b)诊断与管理;(c)团队合作与管理;(d)沟通;(e)职业行为;(f)职业价值观。这些发现与中国相关,符合其当前情况,并且与其他国家所开发的类似。