Tousignant-Laflamme Yannick, Beaudoin Ann-Marie, Renaud Anne-Marie, Lauzon Stephanie, Charest-Bossé Marie-Catherine, Leblanc Louise, Grégoire Maryse
School of Rehabilitation, Université de Sherbrooke, Sherbrooke, QC, Canada.
Centre de recherche Clinique du CHUS (CRCHUS), Sherbrooke, QC, Canada.
BMC Emerg Med. 2015 Dec 3;15:35. doi: 10.1186/s12873-015-0062-1.
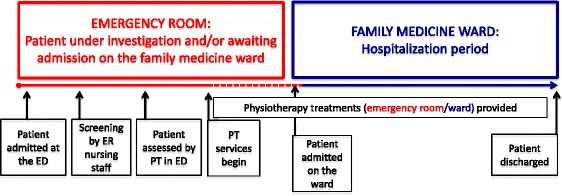
The association between the functional decline occurring with bedrest and hospitalization in older persons is well-known. A long wait in the emergency department (ED), where patients can be bedridden, is a risk factor for the development of an immobilization syndrome (IS). IS is one of the unwanted consequences of inactivity, which causes pathological changes in most organs and systems. Early mobility interventions, such as physical therapy (PT) delivered in the ED, may prevent its development. To our knowledge, no prior studies have reported on this topic. The goal of this study was to (i) assess the feasibility and (ii) explore the potential clinical value of adding PT services to the ED, in collaboration with nursing staff, to prevent IS.
For 12 weeks, PT services were delivered in the ED to older persons (>65 years old) presenting with ≥1 clinical signs associated with the development of IS. Patients were screened by ED nurses and then seen by the physiotherapist. In order to assess feasibility, access to patients, percentage of patients who met eligibility criteria, acceptability of the intervention, and barriers/facilitators to the implementation were measured. To describe the clinical benefits of early PT services, we counted the number of new IS cases among patients after their admission to the ward.
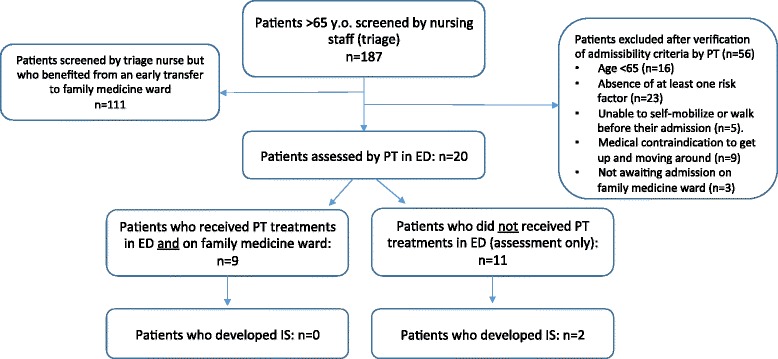
After 12 weeks, the ED nurses screened 187 potential patients and 20 received PT services in the ED (before their admission to the ward). Accessibility was not an issue and we observed good acceptability from the milieu. We did not find majors problems or insurmountable obstacles to implementation of the intervention. Clinical outcomes showed that nine patients received PT treatments in the ED and on the ward (after their admission). For the 11 other patients, no PT interventions were done in the ED following the assessment. Follow-up of these 11 patients showed that two of them developed IS during their hospital stay. As for the nine patients who began PT treatments in the ED, none of them developed IS.
Based on the results of this feasibility study, it would be likely and potentially beneficial to implement PT services in the ED, which could have a positive impact on preventing the development of IS in older persons presenting risk factors. While only a small proportion of patients (11 %) received PT services, better screening tools/methods should be developed.
老年人卧床休息和住院期间出现的功能衰退之间的关联是众所周知的。在急诊科(ED)长时间等待,患者可能会卧床不起,这是发生制动综合征(IS)的一个危险因素。IS是不活动的不良后果之一,会导致大多数器官和系统发生病理变化。早期活动干预,如在急诊科提供物理治疗(PT),可能会预防其发生。据我们所知,此前尚无关于该主题的研究报告。本研究的目的是:(i)评估可行性;(ii)探讨与护理人员合作在急诊科增加PT服务以预防IS的潜在临床价值。
在12周内,对出现≥1种与IS发生相关临床体征的老年人(>65岁)在急诊科提供PT服务。患者由急诊科护士进行筛查,然后由物理治疗师进行诊治。为了评估可行性,测量了患者的可及性、符合入选标准的患者百分比、干预的可接受性以及实施的障碍/促进因素。为了描述早期PT服务的临床益处,我们统计了患者入院病房后新发生IS的病例数。
12周后,急诊科护士筛查了187名潜在患者,其中20名在急诊科接受了PT服务(在入院病房之前)。可及性不是问题,我们观察到环境具有良好的可接受性。我们没有发现实施干预存在重大问题或不可逾越的障碍。临床结果显示,9名患者在急诊科和病房(入院后)接受了PT治疗。对于其他11名患者,评估后在急诊科未进行PT干预。对这11名患者的随访显示,其中2名在住院期间发生了IS。至于在急诊科开始PT治疗的9名患者,他们中没有人发生IS。
基于这项可行性研究的结果,在急诊科实施PT服务可能是可行的且潜在有益的,这可能对预防有危险因素的老年人发生IS产生积极影响。虽然只有一小部分患者(11%)接受了PT服务,但应开发更好的筛查工具/方法。