Horvatits Thomas, Kneidinger Nikolaus, Drolz Andreas, Roedl Kevin, Rutter Karoline, Kluge Stefan, Trauner Michael, Fuhrmann Valentin
Division of Gastroenterology and Hepatology, Department of Internal Medicine 3, Medical University of Vienna, Vienna, Austria.
Department of Intensive Care Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
Ann Intensive Care. 2015 Dec;5(1):47. doi: 10.1186/s13613-015-0092-6. Epub 2015 Dec 4.
Hepatic impairment is found in up to 20 % in critically ill patients. Hypoxic/ischemic hepatitis (HH) is a diffuse hepatic damage associated with high morbidity and mortality. Indocyanine green plasma disappearance rate (ICG-PDR) is an effective tool assessing liver function in acute and chronic hepatic diseases. Aim of this study was to evaluate the prognostic impact of ICG-PDR in comparison to established parameters for risk stratification.
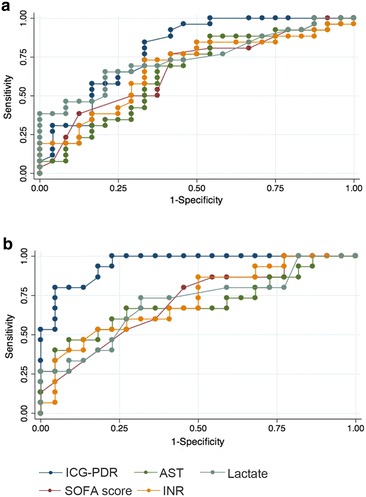
Patients with HH were included in this prospective observational study and compared to cirrhosis, acute liver failure (ALF) and patients without underlying liver disease. ICG-PDR, measured non-invasively by finger pulse densitometry, was assessed on admission and in patients with HH serially and results were compared between groups. Diagnostic test accuracy of ICG-PDR predicting 28-day mortality was analyzed by receiver operating characteristics (ROC).
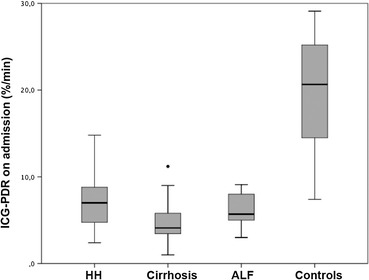
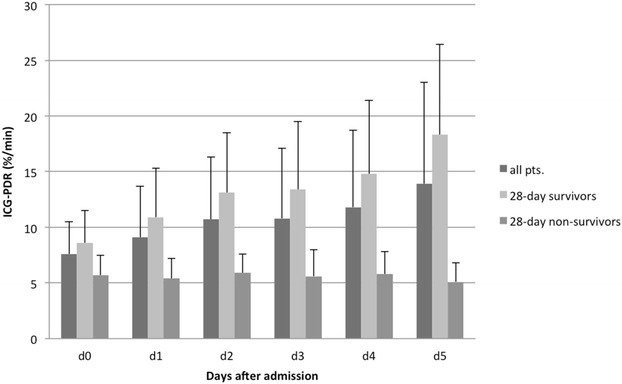
ICG-PDR on admission was significantly lower in patients with liver diseases than in patients without hepatic impairment (median 5.7 %/min, IQR 3.8-7.9 vs. 20.7 %/min, IQR 14.1-25.4 %/min; p < 0.001). ICG-PDR predicted 28-day mortality independently of SOFA score and serum lactate in patients with underlying liver disease (HR 1.27, 95 % CI 1.10-1.45, p < 0.001). In patients with HH, ICG-PDR was identified as best predictor of 28-day mortality which performed significantly better than SOFA, lactate, INR and AST over course of time (p < 0.05). Best cut-off for identification of 28-day survivors was ICG-PDR ≥9.0 %/min 48 h after admission.
ICG-PDR is an independent predictor of mortality in patients with liver disease. Diagnostic test accuracy of ICG-PDR was superior to standard liver function parameters and established scoring systems in patients with HH.
危重症患者中高达20%存在肝功能损害。缺氧/缺血性肝炎(HH)是一种弥漫性肝损伤,发病率和死亡率都很高。吲哚菁绿血浆消失率(ICG-PDR)是评估急慢性肝病肝功能的有效工具。本研究的目的是评估ICG-PDR与既定风险分层参数相比的预后影响。
HH患者纳入本前瞻性观察性研究,并与肝硬化、急性肝衰竭(ALF)患者以及无潜在肝病的患者进行比较。通过手指脉搏密度测定法无创测量ICG-PDR,在入院时对HH患者进行连续评估,并比较各组结果。采用受试者工作特征曲线(ROC)分析ICG-PDR预测28天死亡率的诊断试验准确性。
肝病患者入院时的ICG-PDR显著低于无肝功能损害的患者(中位数5.7%/分钟,四分位间距3.8 - 7.9 vs. 20.7%/分钟,四分位间距14.1 - 25.4%/分钟;p < 0.001)。在有潜在肝病的患者中,ICG-PDR独立于序贯器官衰竭评估(SOFA)评分和血清乳酸预测28天死亡率(风险比1.27,95%置信区间1.10 - 1.45,p < 0.001)。在HH患者中,ICG-PDR被确定为28天死亡率的最佳预测指标,在整个病程中其表现明显优于SOFA评分、乳酸、国际标准化比值(INR)和天门冬氨酸氨基转移酶(AST)(p < 0.05)。识别28天存活者的最佳截断值是入院后48小时ICG-PDR≥9.0%/分钟。
ICG-PDR是肝病患者死亡率的独立预测指标。在HH患者中,ICG-PDR的诊断试验准确性优于标准肝功能参数和既定评分系统。