Leonhardt Silke, Veltzke-Schlieker Wilfried, Adler Andreas, Schott Eckart, Eurich Dennis, Faber Wladimir, Neuhaus Peter, Seehofer Daniel
From the Department of General, Visceral and Transplantation Surgery, Charité-Universitätsmedizin Berlin, Augustenburger Platz 1, Berlin, Germany (SL, DE, WF, PN, DS); Endoscopy Unit, Department of Gastroenterology and Hepatology, Endocrinology, Diabetes and Metabolic Diseases, Charité-Universitätsmedizin Berlin, Augustenburger Platz 1, Berlin, Germany (WV-S, AA, ES); and Department of Gastroenterology, Hepatology and Infectious Diseases, Heinrich-Heine-University Düsseldorf, Moorenstrasse 5, Düsseldorf, Germany (SL).
Medicine (Baltimore). 2015 Dec;94(49):e2188. doi: 10.1097/MD.0000000000002188.
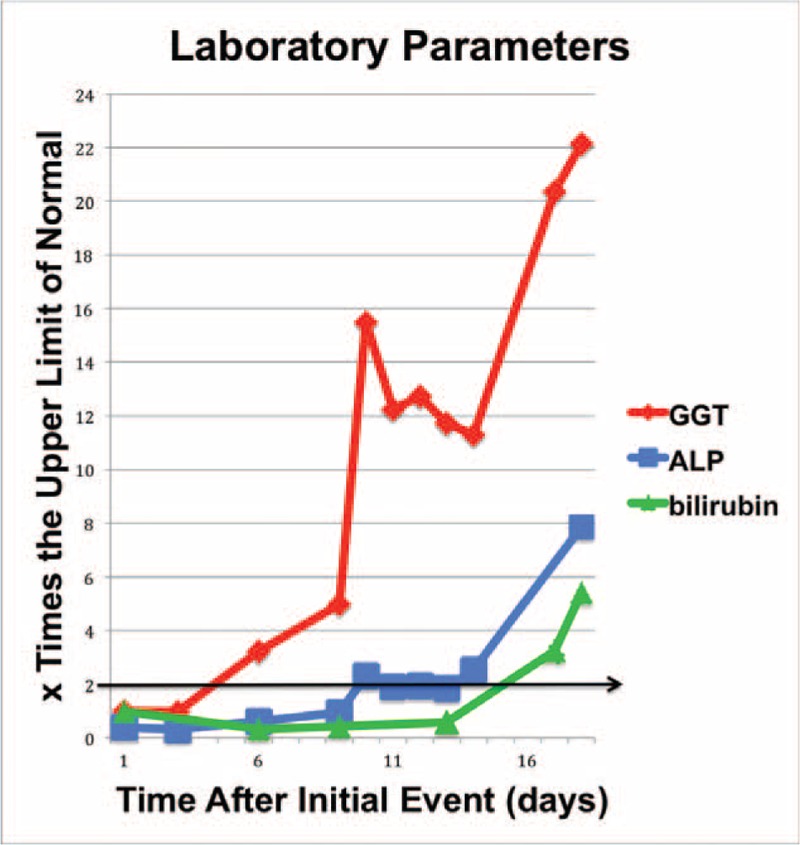
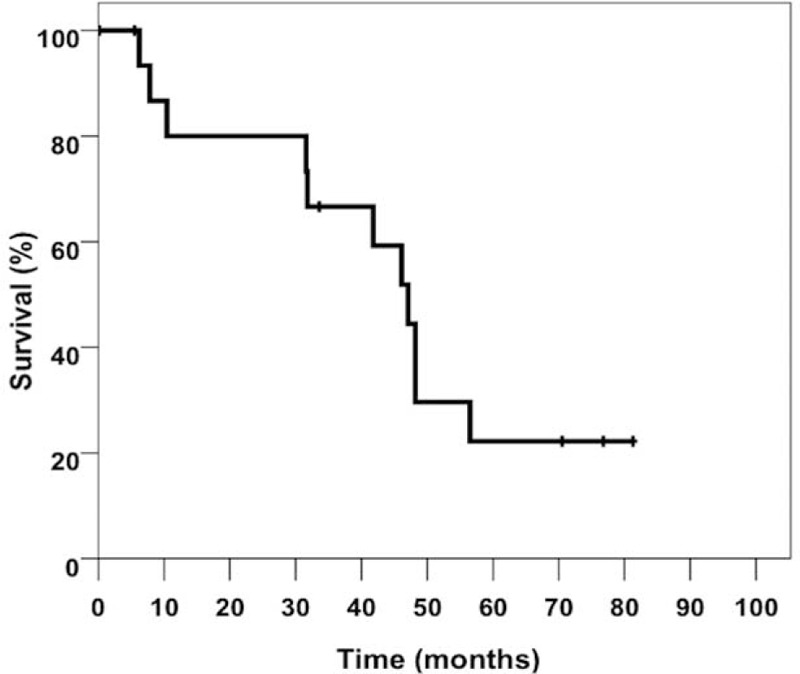
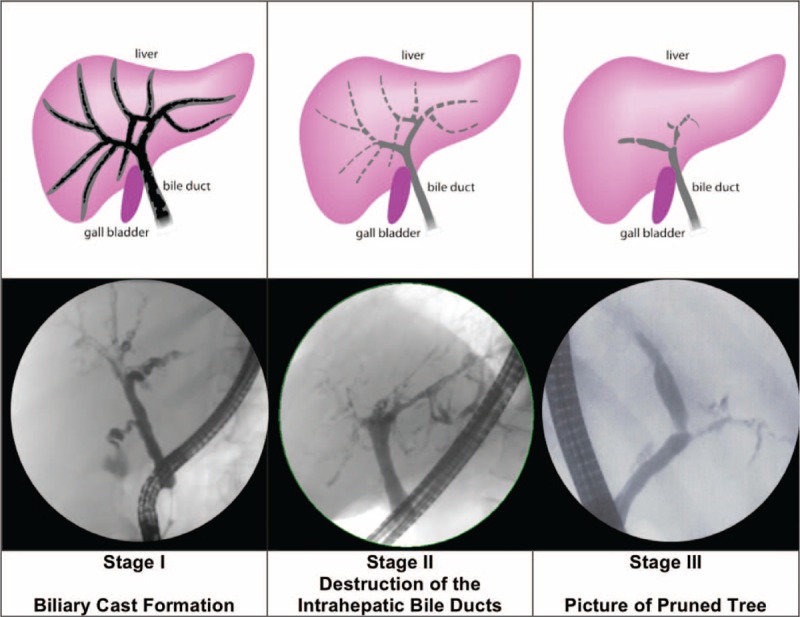
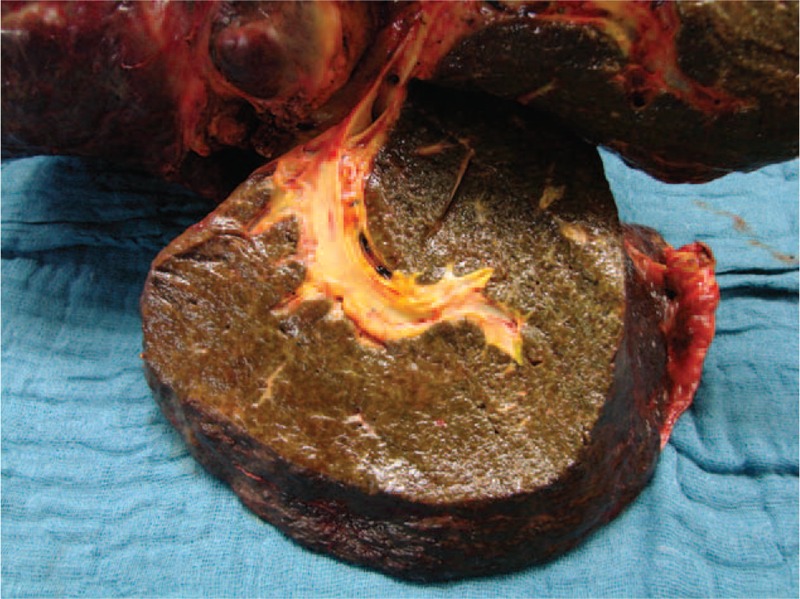
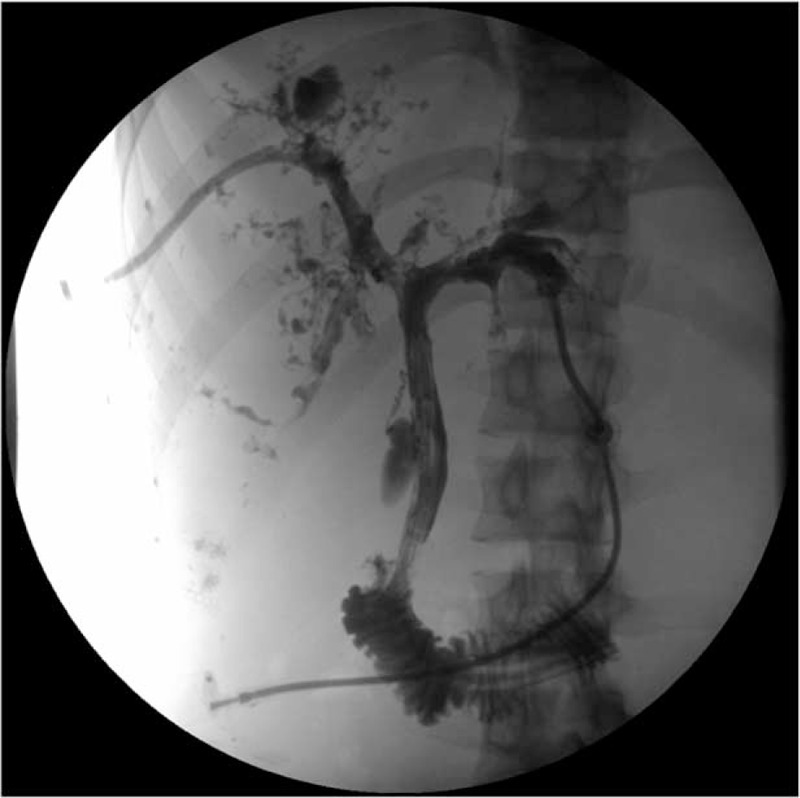
Secondary sclerosing cholangitis in critically ill patients (SSC-CIP) is an important differential diagnosis in patients presenting with cholestasis and PSC-like cholangiographic changes in endoscopic retrograde cholangiography (ERC). As a relatively newly described entity, SSC-CIP is still underdiagnosed, and the diagnosis is often delayed. The present study aims to improve the early detection of SSC-CIP and the identification of its complications.A total of 2633 records of patients who underwent or were listed for orthotopic liver transplantation at the University Hospital Charité, Berlin, were analyzed retrospectively. The clinical presentation and outcome (mean follow-up 62.7 months) of the 16 identified SSC-CIP cases were reviewed.Cholestasis was the first sign of SSC-CIP. GGT was the predominant enzyme of cholestasis. Hypercholesterolemia occurred in at least 75% of the patients. SSC-CIP provoked a profound weight loss (mean 18 kg) in 94% of our patients. SSC-CIP was diagnosed by ERC in all patients. The 3 different cholangiographic features detected correspond roughly to the following stages: (I) evidence of biliary casts, (II) progressive destruction of intrahepatic bile ducts, and (III) picture of pruned tree. Biliary cast formation is a hallmark of SSC-CIP and was seen in 87% of our cases. In 75% of the patients, the clinical course was complicated by cholangiosepsis, cholangitic liver abscesses, acalculous cholecystitis, or gallbladder perforation. SSC-CIP was associated with worse prognosis; transplant-free survival was ∼40 months (mean).Because of its high rate of serious complications and unfavorable prognosis, it is imperative to diagnose SSC-CIP early and to differentiate SSC-CIP from other types of sclerosing cholangitis. Specific characteristics enable identification of SSC-CIP. Early cooperation with a transplant center and special attention to biliary complications are required after diagnosis of SSC-CIP.
危重症患者的继发性硬化性胆管炎(SSC-CIP)是在内镜逆行胆管造影(ERC)中出现胆汁淤积和类似原发性硬化性胆管炎(PSC)胆管造影改变的患者的重要鉴别诊断。作为一个相对新描述的实体,SSC-CIP仍未得到充分诊断,诊断往往延迟。本研究旨在提高SSC-CIP的早期检测及其并发症的识别。对柏林夏里特大学医院接受原位肝移植或被列入移植名单的2633例患者的记录进行了回顾性分析。对16例确诊的SSC-CIP病例的临床表现和结局(平均随访62.7个月)进行了评估。胆汁淤积是SSC-CIP的首发症状。γ-谷氨酰转肽酶(GGT)是胆汁淤积的主要酶。至少75%的患者出现高胆固醇血症。SSC-CIP使94%的患者体重显著减轻(平均18千克)。所有患者均通过ERC诊断出SSC-CIP。检测到的3种不同胆管造影特征大致对应以下阶段:(I)胆管铸型证据,(II)肝内胆管进行性破坏,以及(III)枯树枝样表现。胆管铸型形成是SSC-CIP的标志,在87%的病例中可见。75%的患者临床病程并发胆管败血症、胆管性肝脓肿、无结石性胆囊炎或胆囊穿孔。SSC-CIP与较差的预后相关;无移植生存期约为40个月(平均)。由于其严重并发症发生率高且预后不良,早期诊断SSC-CIP并将其与其他类型的硬化性胆管炎区分开来至关重要。特定特征有助于识别SSC-CIP。诊断SSC-CIP后需要与移植中心早期合作并特别关注胆道并发症。