Colivicchi Furio, Sternhufvud Catarina, Gandhi Sanjay K
Cardiology Division, Emergency Department, San Filippo Neri Hospital, ASL Roma E, Rome, Italy.
Global Payer Evidence and Pricing, AstraZeneca R&D, Mölndal, Sweden.
Clinicoecon Outcomes Res. 2015 Nov 27;7:555-65. doi: 10.2147/CEOR.S88817. eCollection 2015.
No clinical trials have been conducted to directly compare the effect of the two high-intensity statins, rosuvastatin and atorvastatin, on cardiovascular outcomes. However, three such trials have been computer-simulated using the Archimedes model, an individual-based simulation of human physiology and behaviors, treatment interventions, and health care systems. The results are reviewed here.
The first simulated trial assessed clinical outcomes in patients receiving available doses of the two drugs. The second assessed the impact of initial treatment decisions, while the third assessed the effect of switching from rosuvastatin to atorvastatin.
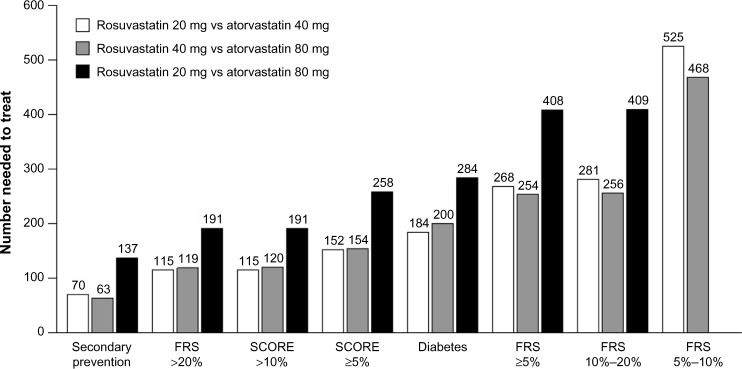
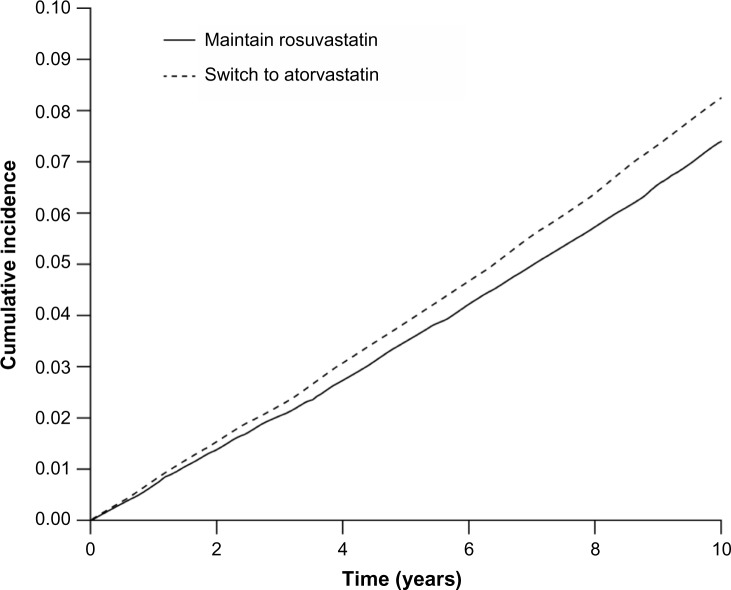
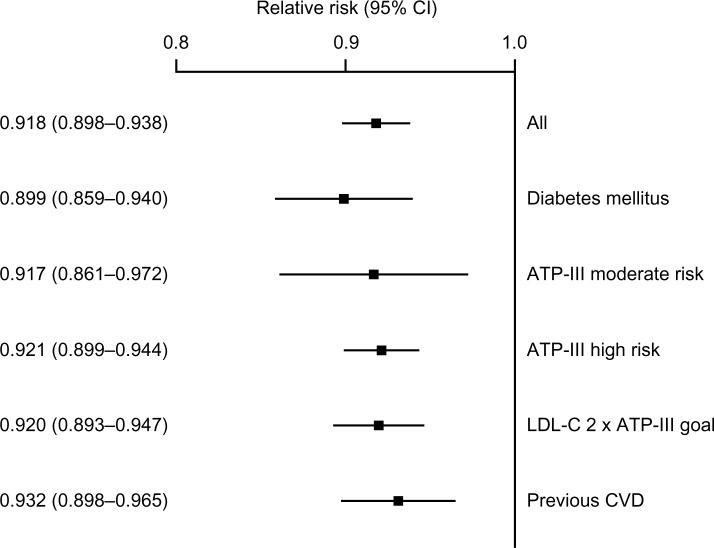
In the first simulated trial, treatment with rosuvastatin was estimated to result in greater reductions than treatment with atorvastatin in major adverse cardiac event (MACE) rates at 5 years and 20 years at all doses examined (relative risk [RR]: 0.897, 0.888, and 0.930 at 5 years for rosuvastatin 20 mg vs atorvastatin 40 mg, rosuvastatin 40 mg vs atorvastatin 80 mg, and rosuvastatin 20 mg vs atorvastatin 80 mg, respectively; all P<0.05). In the second simulated trial, outcomes were significantly better in patients initially prescribed rosuvastatin than in those initially prescribed atorvastatin (RR of MACE at 5 years: 0.918; P<0.001). In the third simulated trial, risk of MACE was significantly greater in patients switching from rosuvastatin to atorvastatin than in those remaining on rosuvastatin (RR at 5 years: 1.109; P<0.001).
The results of these simulated clinical trials suggest improved outcomes among patients receiving rosuvastatin relative to patients receiving atorvastatin in various clinical settings.
尚未进行临床试验直接比较两种高强度他汀类药物(瑞舒伐他汀和阿托伐他汀)对心血管结局的影响。然而,已使用阿基米德模型对三项此类试验进行了计算机模拟,该模型是基于个体的人类生理与行为、治疗干预及医疗保健系统的模拟。在此对结果进行综述。
第一项模拟试验评估接受两种药物可用剂量的患者的临床结局。第二项评估初始治疗决策的影响,而第三项评估从瑞舒伐他汀换用阿托伐他汀的效果。
在第一项模拟试验中,在所有检测剂量下,估计瑞舒伐他汀治疗在5年和20年时导致的主要不良心脏事件(MACE)发生率降低幅度大于阿托伐他汀治疗(5年时,瑞舒伐他汀20 mg对比阿托伐他汀40 mg、瑞舒伐他汀40 mg对比阿托伐他汀80 mg、瑞舒伐他汀20 mg对比阿托伐他汀80 mg的相对风险[RR]分别为0.897、0.888和0.930;均P<0.05)。在第二项模拟试验中,初始处方瑞舒伐他汀的患者的结局显著优于初始处方阿托伐他汀的患者(5年时MACE的RR:0.918;P<0.001)。在第三项模拟试验中,从瑞舒伐他汀换用阿托伐他汀的患者发生MACE的风险显著高于继续使用瑞舒伐他汀的患者(5年时RR:1.109;P<0.001)。
这些模拟临床试验的结果表明,在各种临床环境中,接受瑞舒伐他汀治疗的患者相对于接受阿托伐他汀治疗的患者结局有所改善。