Kingsley Jeff, Mehra Purvi, Lawrence Laura E, Henry Eugenia, Duffy Erin, Cammarata Sue K, Pullman John
Columbus Regional Research Institute, 800 Talbotton Road, Columbus, GA 31904, USA.
Artemis Institute for Clinical Research, 770 Washington St., San Diego, CA 92103, USA.
J Antimicrob Chemother. 2016 Mar;71(3):821-9. doi: 10.1093/jac/dkv411. Epub 2015 Dec 17.
Delafloxacin is an investigational anionic fluoroquinolone being developed to treat infections caused by Gram-positive and -negative organisms. This clinical trial evaluated the efficacy and safety of delafloxacin in the treatment of acute bacterial skin and skin structure infections (ABSSSIs).
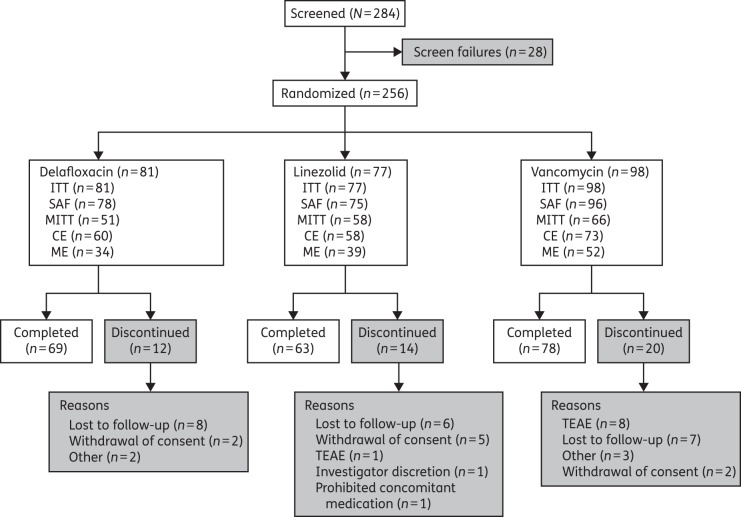
In a double-blind, Phase 2 trial, 256 patients were randomized (1 : 1 : 1) to 300 mg of delafloxacin, 600 mg of linezolid or 15 mg/kg vancomycin (actual body weight), each administered intravenously twice daily for 5-14 days. Randomization was stratified by infection category. The primary endpoint was the investigator's assessment of cure, defined as complete resolution of baseline signs and symptoms at follow-up. Secondary endpoints included reductions in the total areas of erythema and induration and assessments of bacterial eradication. This trial has been registered at ClinicalTrials.gov under registration number NCT01283581.
Cure rates were significantly greater with delafloxacin versus vancomycin (mean difference: -16.3%; 95% CI, -30.3% to -2.3%; P = 0.031); differences were significant for obese patients (BMI ≥30 kg/m(2); mean difference: -30.0%; 95% CI, -50.7% to -9.3%; P = 0.009), but not for non-obese patients. Cure rates with delafloxacin and linezolid were similar. Using digital measurement, the percentage decrease in total erythema area was significantly greater with delafloxacin versus vancomycin at follow-up (-96.4% versus -84.5%; P = 0.028). There were no differences in bacterial eradication among the treatment groups. The most frequently reported treatment-emergent adverse events were nausea, diarrhoea and vomiting.
These data show that delafloxacin is effective in the treatment of ABSSSIs and is well tolerated.
德拉氟沙星是一种正在研发的阴离子氟喹诺酮类药物,用于治疗革兰氏阳性和阴性菌引起的感染。本临床试验评估了德拉氟沙星治疗急性细菌性皮肤及皮肤结构感染(ABSSSI)的疗效和安全性。
在一项双盲2期试验中,256例患者按1∶1∶1随机分为三组,分别接受300mg德拉氟沙星、600mg利奈唑胺或15mg/kg万古霉素(实际体重)治疗,均静脉注射,每日2次,疗程5 - 14天。随机分组按感染类别进行分层。主要终点为研究者对治愈情况的评估,定义为随访时基线体征和症状完全消失。次要终点包括红斑和硬结总面积的缩小以及细菌清除情况的评估。本试验已在ClinicalTrials.gov注册,注册号为NCT01283581。
德拉氟沙星组的治愈率显著高于万古霉素组(平均差异:-16.3%;95%CI,-30.3%至-2.3%;P = 0.031);肥胖患者(BMI≥30kg/m²)中差异显著(平均差异:-30.0%;95%CI,-50.7%至-9.3%;P = 0.009),而非肥胖患者中差异不显著。德拉氟沙星组和利奈唑胺组的治愈率相似。采用数字测量法,随访时德拉氟沙星组红斑总面积的下降百分比显著高于万古霉素组(-96.4%对-84.5%;P = 0.028)。各治疗组在细菌清除方面无差异。最常报告的治疗中出现的不良事件为恶心、腹泻和呕吐。
这些数据表明,德拉氟沙星治疗ABSSSI有效且耐受性良好。